

Torso Wound Care Page Menu: 1 2 3 4 5 6 7 8 9 10 Next>>
Torso Wound Care During the Golden Age of Piracy, Page 4
Wounds of the Thorax - Complications: Trapped Substances
One critical complication of a penetrating chest wound was when substances remained inside the wound. The majority of these substances were fluids such as blood, serum and pus.
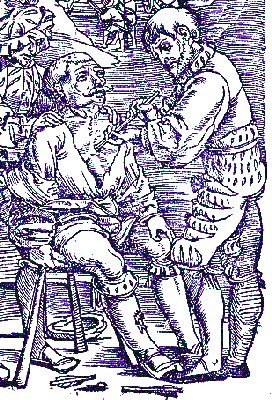
Artist: Hans von Gersdorf
Withdrawing Fluid From a Chest Wound (1530)
From the
Wellcome Collection
Sea surgeon John Woodall explained "Wounds that penetrate the inward parts are dangerous, namely, if any great quantitie of bloud lie in the capacity of the Thorax, which cannot be evacuated by the wound, but if it can be evacuated there is hope, otherwise it is desperate."1 Woodall went on to say that if the blood could be extracted and the internal organs were not damaged, the wound could be healed provided the surgeon was careful not to allow air to enter into it. Since the issues associated with failing to drain fluids from chest wounds have already been discussed in some detail we will not dwell upon this, but will instead focus on methods for extracting fluids which are trapped.
The easiest way to extract the blood was by non-surgical means. French surgical instructor Pierre Dionis, who devoted an entire section of his book to this problem, provided several suggests for accomplishing this, recommending that the surgeon start with the 'gentlest' means first. His first recommendation is the most straight-forward: "placing the Patient in such a manner, that the Blood may run out of the Wound, which is done by obliging him to incline his Head downwards, raising up his Thighs, and laying him on the Wound it self"2.
His second suggestion is a little more challenging for the patient; "to assist the Blood in its issuing out, by closing the Patient's Nose, ordering him to hold his Breath a little, and also shaking the Body a little"3. It can readily be seen how uncomfortable this would have been for someone freshly wounded in the chest.
His final suggestion was to use an instrument he initially refers to as a pyulcon, which is a device briefly mentioned by 1st/2nd AD physician Galen of Pergamon. It is essentially a metal syringe "whose Pipe is bent to accommodate it to the Shape of the Wound...
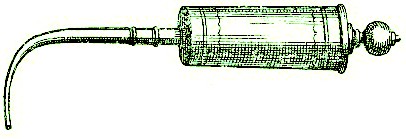
Pyulcon or Fluid Extraction Syringe From Cours d'Operations,
By
Pierre Dionis, p. 291 (1708)
[which by] drawing out the handle of the Syringe, the Chirurgeon thereby fills it with this extravasated [leaking] Humour, and thus sucks or pumps it several times."4
Richard Wiseman also mentions three methods which period physicians thought could eject humors of such wounds: "by the Mouth, by Expectoration [coughing]; or by the Wound; or by Urine."5 With the exception of removal via the wound, these methods would all have involved the use of medicines: emetics to create vomiting (by mouth), expectorants to encouraging coughing and diuretics to encourage urination. Wiseman was skeptical of using urine as a vehicle for extracting blood from a chest wound, however. "[I]f the matter of fact be true, that there is sometimes a discharge by Urine, ...I confess I have not observed in my own practice"6.
Wiseman does offer suggestions for expectorants, such as

Photo: Kurt Stueber - Maidenhair (Asplenium trichomanes)
decoct. pectoral [Decoction Pectoral, containing barley, raisins, figs, liquorice roots and water], Lochochs ['lickable' medicines], syr. capill[arum] ven[eris]. [syrup of maidenhair] jujub[e]. glycyrriz. [licorice] oxymel [honey], &c. whereof the Pharmacopœia Lond[inensis]. is full.7
French surgeon Ambroise Paré spends a great deal of time discussing the problem of fistulas, which can have fluids trapped in them. He notes that fistulas are basically ulcers with cavities in them.8 This is even better explained by apothecary John Quincy. He says that while a fistula is any kind of pipe in the skin, "its most common Use [as a word] is for Ulcers that lie deep, and ouze out their Matter thro’ long, narrow, winding Passage"9. It is because of this 'oozing matter' that healing them was so important.
Paré warns that "Fistula’s of the Chest, are scarse cured at any time, and that for divers causes."10 He lists three such causes: a) the continuous motion of the chest, b) their location in a membrane covering the ribs which contains no blood (while bad blood humors could delay healing, good blood humors were required to encourage it) and c) the wound in the membrane cannot be sutured which hinders the edges from rejoining.11Despite these problems, Paré suggests that there is some possibility that the wound can be healed.
Healing is accomplished in part through the use of humoral-based methods such as bloodletting and diet as well as the application of healing medicines (vulneraries). Paré recommends injecting the following such medicines into the fistulas:

Photo: Wiki User Hectonichus - Aristolochia rotunda
the powders of Aloes, Gentian [root], Aristolochia, centaury, cortex pini [pine bark], as Rx. radic. Ireos Flor. [roots of iris Florentini] aristolochiæ {of each, 1 dram}, corticis pini [pine bark] {1/2 dram}, Misce & fiat pulvis [mix and make into a powder]12
This powder is to be added to syrup of dried roses and honey of roses. "Neither do I, if the putrefaction be great, fear to mix therewith Ægyptiacum."13 These medicines were to prevent deterioration in the wound. Paré warns the reader,
you must have a care to remember & observe the quantity of the injected liquor, that you may know whether it all come forth again after it hath performed its detergent [cleansing] office. For if any thereof remain behind in the corners and crooked passages, it hurts the part, as corrupted with the contagion thereof.14
Here again we see the problem of fluids remaining in the wound. Once cleansed, Paré recommends healing the fistula. With this in mind,

Photo: Wiki User Dalgial - Knotgrass (Polygonum aviculare)
you must command the Patient to use emplastick [adhesive], austere, and astringent medicines, such as are Terra sigillata [sealed earth], bolus armenus [Armenian earth], hypocystis [Cytinus hypocistis], plantain [plantago], knot-grass [polygonum], Sumach, acacia and the like, which the Patient shall use in his broaths and Eclegma’s [thick medicinal juices], mixing therewith honey of roses, which serving for a vehicle to the rest, may carry away the impacted filth which hinders agglutination.15
In addition to the problem of fluids, military surgeon Richard Wiseman discusses the problem of an air-filled tumor forming at the wound site. Wiseman explains in a case study that he "felt the swelled Parts crackle under my fingers. Concluding it Wind got out from the Cavity within the Thorax, I made incision into the Swelling about an inch long, which the Wind was discharged."16 He then applied turpentine to the wound, and kept it "open two or three Dressings [with a piece of cloth or dossil], till the Penetration into the Breast was incarned [new flesh formed in the wound]; then lessened the Dossil, and healed it"17.
1 John Woodall, the surgions mate, 1617, p. 139; 2,3,4 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., 1733, p. 233; 5 Richard Wiseman, Of Wounds, Severall Chirurgicall Treatises, 1686, p. 366; 6,7 Wiseman, p. 367; 8 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 2; 9 John Quincy, Lexicon Physio-Medicum, 1726, p. 168; 10,11 Paré, p. 298; 12 Paré, p. 286; 13,14 Paré, p. 298; 15 Paré, p. 298; 16,17 Wiseman,p. 368
Pierre Dionis' Empyema Surgery
If none of these methods can adequately drain fluids from wounds of the chest, Pierre Dionis
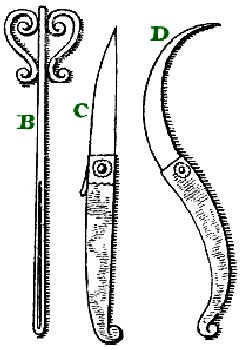
Chest Dilation Tools From Cours d'Operations,
By
Pierre Dionis, p. 291 (1708)
advises a surgical method. He notes "that is done two ways, either by dilating [enlarging] the Wound, or by making a Counter-Aperture [a second incision]."1 As befits an instructor, Dionis provides a thorough explanation of the procedure with accompanying graphics.
The Wound is to be dilated, when the Orifice is in the lower part of the Breast, either before or behind... which is done by thrusting the hollow Probe B into the Wound, in order to guide in the Point of an Instrument, which must be either the strait Incision Knife C, or a crooked Pen-knife D; and we must observe, that we always make the Incisions downwards on the Teguments [epidermis] and exterior Muscles, to facilitate the issuing out of the Blood.2
Note that he is careful not to make the incision too deeply for fear of damaging the organs. If the wound was in the upper part of the chest, Dionis advised against enlarging the existing wound, ordering instead that the surgeon "must of necessity make a Counter-Aperture, which is what we call the Empyema."3
It should be noted that Dionis' definition of 'empyema' is different than that in normal use, even by other surgeons during this period. In his text this word refers to the operation whereby a second incision is made in the chest to allow fluids to flow out. In the normal medical parlance, empyema is not an operation, but is defined as "a Collection of Matter in any Part whatsoever; strictly taken: but it is generally used to signify that in the Cavity of the Breast only"4. However, for the duration of this section, 'empyema' refers to Dionis' operation.
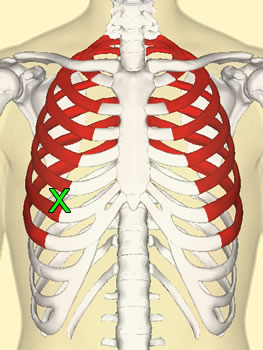
X - Approximate Location of Incision in
Front of Chest
Dionis explains that the second incision "is made on the Declivity [downward slope], or inclining [?] part of the Breast, in two places, viz. in the fore, or hind-part."5 He goes on to explain the location more thoroughly. In the front, it is made "betwixt the second and third of the Costa-vera, or
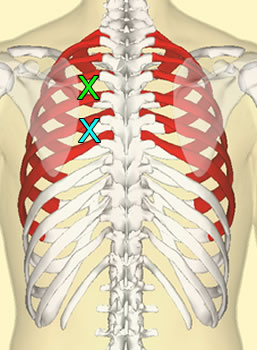
X - Location of Incision in Back of Chest
It seems likely that Dionis miscounted or
misrepresented the rib count
based on the
second description, which would be closer to X.
long Ribs [colored red in these images], telling [counting] them upwards; this Method affords the Patient the advantage of being able to dress himself, when he is obliged to quit his Chirurgeon."6
However, Dionis also says this incision is inconvenient because the patient must lie on his stomach to drain fluids from the wound. He prefers making the incision in the back, advising that with this incision "the Matter easily repairs to the Orifice, and issues out without doing any Violence to the Lungs."7 When making the incision in the back, the surgeon places "his Incision Knife betwixt the third and fourth of the Vera-costa, or long Ribs, reckoning upwards, that is, one Rib higher than before, in order to avoid the Diaphragma"8. In case the surgeon doesn't want to count ribs, he further explains the location on the back, telling the surgeon he can "make the Incision four Fingers breadth below the Angle of the Omoplata [scapula], and the same breadth from the Spina [spine]"9. The description of these two locations do not appear to agree with one another, however. This may be because of the way Dionis is counting ribs.
Dionis then describes the operation, using his preferred location in the back.
From Johannes Scultetus, l'Arcenal de Chirurgie (1665)
After having turn'd his [the patient's] Back towards the Light, and taken up his Shirt, he [the surgeon] pinches the Teguments [epidermis] at the place which he designs to open, and causes them to be held with one hand by a Servant, at the same time raising them with his Left-hand, with his right he cuts them with the strait Incision Knife C; when having loosen'd the Teguments, he compleats the crossing the Muscles betwixt two Ribs, turning the Back of his Incision Knife towards the upper Rib, in order to avoid piercing the Vessels which are situate[d] along the lower part of that Bone. The Muscles being cut, he opens the Pleura [membrane covering the lungs] with the Point of the same Instrument, which he then draws out to thrust in his Finger, in order to know whether the Orifice is sufficient: After which, he causes the Patient to be laid on his Back, to facilitate the coming out of the Blood, which ordinarily runs forth abundantly10
Once the fluid had drained, the surgeon dressed the wound using a Tent (E). Dionis says that this tent should be: a) proportioned to the size of the wound; b) soft; c) short and blunt (F) to avoid damaging the Lungs; d) flattened so that it will fit between the ribs; e) made with a
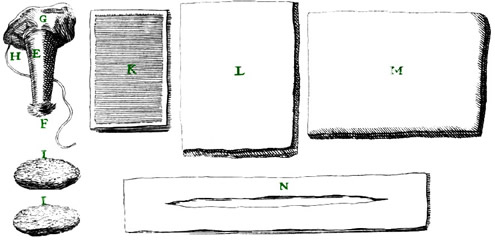
Empyema Operation Dressings From Cours d'Operations, By
Pierre Dionis, p. 291 (1708)
'head' (G) so that it doesn't fall into the incision and have a string (H) so it can be pulled back out if it does; and f) soaked in a vulnerary or healing medicine. Note that these are all properties which were stated by other authors in the section on using tents in wounds of the chest cavity.
Like other wounds of the chest, Dionis recommends that the surgeon embrocate "all around the Wound, which he [the surgeon] covers with the flat Pledgets I I, and a large Plaister, K, of Gratia Dei [The Grace of God Plaster - made of turpentine, pitch, white wax, mastic, betony, vervain and burnet]."11On top of this is placed a square compress (L), a roller bandage to hold it in place and a 'Napkin' (M), " folded in three or four Pleats, which is securely kept in its place, by fastening it to the scapulary Bandage N, before or behind."12
Dionis states that the wound must be allowed to drain whenever the patient feels 'oppressed', which can be as as soon as six to eight hours after the new incision is made. 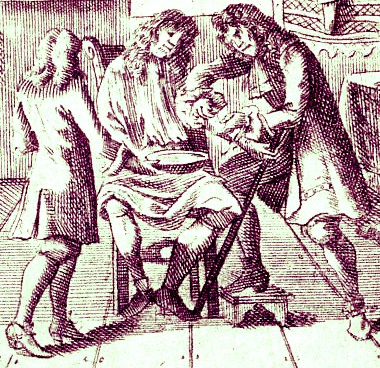
Artist: Wolf Helmhardt von Hohberg - Bleeding a Patient (1695)
"Wherefore the Chirurgeon should have his Apparatus ready to dress the Patient as many times as Necessity requires: Above all, he must not spare bleeding him in the Arm, that by that sort of Revolution he may divert that Humour from issuing out at the Wound."13 The use of 'Revolution in this sentence is incorrect. It is likely that the interpreter of Dionis' work misinterpreted the word for revulsion. Revulsion is the process of bleeding the patient at a place distant from a wound to divert the blood humors away from it.
Dionis also explains that once the new incision is made, the original wound should be allowed to heal closed as soon as it is able. However, he adds that as long as it is open, the original wound is a good place "to make Injections into the Breast, to cleanse and bring off the Pus and moist Sanies [serum, blood and/or pus] which fall thither, we syringe the Patient by the upper Wound, [so that] the Liquors to run out at the lower"14.
Dionis holds this operation in high regard. He finishes his discussion of the operation by explaining that he has found other methods for discharging fluids such as those discussed at the beginning of this section to be inadequate in most cases. "I know that 'tis not impossible that [non-surgical methods for removing fluids to remove] the extravasated [leaking] Humour yet remaining in the Lungs, or in the Pleura... but as soon as the Abscess is broken, and the Pus diffus'd in the Cavity of the Breast, nothing but the Empyema can get it out."15
1,2 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., 1733, p. 233; 3 Dionis, p. 234; 4 John Quincy, Lexicon Pysico-Medicum, 1726, p. 145; 5,6,7,8,9 Dionis, p. 234; 10,11,12 Dionis, p. 235; 13,14 Dionis, p. 236; 15 Dionis, p. 238
Using Drains to Remove Fluids
A couple of surgeons recommend putting drains into wounds to allow fluid discharge during healing. These drains were made of metal, which may explain why the surgeons often call them 'pipes'.
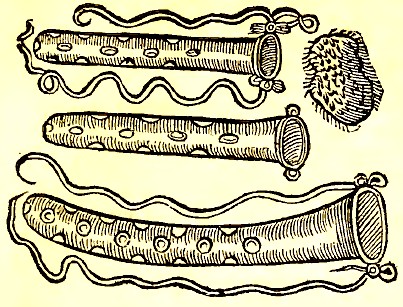
Chest Wound Pipes - Paré notes that the actual pipes "need not have so
many holes as these here exprest; but only two or three in their ends",
From The Workes of That Famous Chirurgeon
Ambrose Parey, p. 299 (1649)
The construction of such drains varied somewhat. Ambroise Paré recommended a pipe in fistulas, advising it be made of gold, silver or lead "and it must have many holes in it, that so the filth may pass forth at them; it must be fast [secured] with strings, that it may not fall into the capacity of the Chest."1 (See image at left.) Instructor Pierre Dionis recommended that in wounds of the breast the surgeon could "make use of a Linten or Linnen Tent; but in that perform’d on occasion of the Rupture of an Abscess, we insert a Silver Pipe"2. For wounds of the lungs which haven't healed within 40 days, James Cooke similarly recommends the surgeon "use a Silver or Lead Pipe; which is to be removed when the Wound runs good matter and little."3
All of them recommended stopping the end of the pipe. Dionis advised using a stopple "to let out as much and as little of the Pus as we think proper"4. Paré recommended a "spunge steeped in aqua vitæ, and wrung forth again ...laid hot to the end of the orifice" to both control the flow of pus as well as prevent air from getting into the wound.5 Emulating Paré , Cooke says, "on it lay a Spunge wrung out of Aq. Vitæ. This keeps out the Air, extracts the Quitter [quitture – fluids coming out of the wound]"6.
Cooke also suggests an alternative to Aqua Vitae, even giving the procedure for preparation, which he says has the ability to draw fluids out of the wound through the pipe:
Rx. Resin rec. Clar. & Odorat [perfumed, rectified and clarified resin]. {1/2 pound} Ol. Laur. [oil of bays] & Tereb. [oil of turpentine] {of each 1 ounce} Gum. Elem. [gum resin of Canarium luzonicum tree] {2 ounces}. First dissolve the Rosin and Gum at a gently Fire, till mixed; after add the Oyle of Turpentine; boyl them a little, strain them through a thick linnen Rag, spread of it on Leather, which being snipt, lay on the Pipe.7
As for the procedure itselff, Dionis gives a detailed explanation of how to install a pipe in a new wound such as the one he made for his empyema operation, again reflecting his role as an instructor.
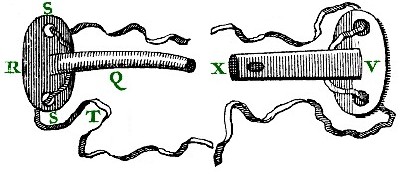
Wound Drains, From Cours d'Operations, By Pierre Dionis, p. 291 (1708)
...the Incision must be made of a proportionate Size to that of the Pipe, which must take up the whole Aperture, and be provided with a Head R, to prevent its slipping into the Breast, and two little holes S S, thro' which to run the string T, which is to run round the Body, that the Pipe may not come out at any other time than when the Operator pleases; when the Ribs are too close, the Body of the Pipe must be flat, like that mark'd V, to adjust it to the spaces betwixt those Bones, and open for the space of its whole length as well as at the fide of its internal extremity X, that the Pus may run off with the greater ease.8
In cases where the pipe was to be installed into an existing wound where the size of the aperture could not be controlled, substances were employed to secure the pipe. German surgeon Matthias Gottfried Purmann says in one of his case studies involving a chest wound that it should be "cover’d with Emplaistr. Andreæ á Cruce"9. This was an adhesive plaster composed of pitch, pine resin, turpentine and oil of bays which served to keep the pipe in place as well as seal it.
Once a drain was installed, Paré explains that the patient can help eject pus and other fluids through the pipe if "often times both day and night he hold his breath, stopping his mouth and nose, and lying upon the diseased side, that so the Sanies may be the more forcibly evacuated"10.
Dionis goes into greater detail, adding steps to the process based on what happened during each treatment.
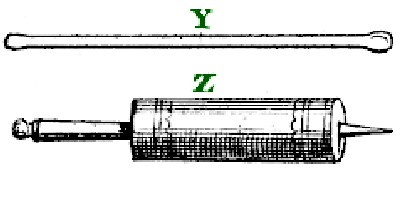
Probe & Syringe, Cours d'Operations, By
Pierre Dionis, p. 291 (1708)
He began by pulling the stopple out of the pipe, "and after having drawn it out, if the Pus don't come out, we must with a large blunt Probe [Y] push back the Lungs, which leaning against the end of the Pipe hinder the desir'd evacuation"11. He then inserted a syringe (Z) into the aperture of the pipe to inject a barley-based medicine mixed with vulnerary plants such as scabiosa (butter bur) or tussilago (coltsfoot) water added to wine and honey of roses. This is used "to cleanse and preserve from Putrefaction (rotting)."12 Dionis suggests injecting the medicine and stopping the orifice "for a moment, then taking out the Stopple, if the Patient incline his Body never so little that way, they issue out at the same Passage."13 He recommends observing the medicine when it is drained back out of the chest cavity, if it
is of an ill Smell and nasty Colour, and is evacuated in great quantity; if the [patient's] Fever continues; if the Patient grows considerably leaner, and his Strength decays, these are all ill-boding Signs; but if the Pus is constantly the same, white, well-digested, of a good Smell, and in small quantity; if the Patient's Strength continues, and he will submit to rules, he will be cur'd14
This is an example of the concept of 'laudible pus' being emitted by a wound, indicating that the bad humors have been removed and the wound can begin properly healing with the help of 'good' humors.
Both Dionis and Paré advise removing the pipe when the discharge lessens. Paré suggests "when it yeelds little, or no matter at all; then it must be cicatrized [healed over with a scar]."15 Dionis warns that this "must be in forty Days, for after that the Wound will degenerate into a Fistula, and require Years to compleat its Cure."16
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 298; 2 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., 1733, p. 240; 3 James Cooke, Mellificium Chirurgiæ: Or, The Marrow of Chiururgery, 1693, p. 131; 4 Paré, p. 298; 5 Dionis, p . 240; 6,7 Cooke, p. 131; 8 Dionis, p . 240; 9 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 130; 10 Paré, p. 298; 11,12,13 Dionis, p . 240; 14 Dionis, p . 240-1; 15 Paré, p. 298; 16 Dionis, p . 241
Torso Wound Care Page Menu: 1 2 3 4 5 6 7 8 9 10 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-