

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 9
Specific Dislocation/Luxation Cure: Wrist
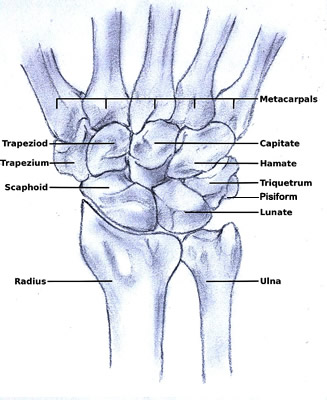
Image: Cvpoucke - Bones Of and Near the Wrist
"It often falls out that the Wrist or Ankle bones are luxated..." (John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 125)
French surgeon Ambroise Paré points out that there are eight bones in the wrist which are held in place on both sides - by the ulna and radius at the back and by the metacarpals in front (shown at left). "Yet may it be dislocated inwardly, outwardly, & towards the sides."1 Like the elbow, Paré refers to 'inward' dislocations which others call 'forward' [pushed out in the direction of the palm of the hand] and outward dislocations which others call backward [pushed out in the direction of the back of the hand].
While every author who talks about how a wrist can be dislocated basically agrees with Paré, sea surgeon John Atkins points out that, based on the structure of the bones in that area, "we may conclude any other Way of Dislocation, than forward or backward improbabl[e]"2. Sea surgeon James Handley narrows it further, stating that the wrist is commonly luxated forward without suggesting the other three ways are common.3
Handley notes that signs of a luxated wrist include a "Tumor on the fore-part, and the Fingers cannot be bent; if it be inward or outward, a Tumor appears on one side, and a Cavity on the other."4 Ambroise Paré adds, "We say it is luxated inwardly [forward] when the hand stands upwards, but [it is luxated] outwardly [backward] , when it is crookt in & cannot be extended."5 Atkins agrees with Handley, stating only that there will be a bump on one side of the wrist and a cavity on the other.6
Reducing and Caring For a Dislocated Wrist
Atkins has little to say about correcting this dislocation, advising only that it is "done easily by Extensions (their [the bones of the wrist] Edges holding still a Part with their Fellows,)..."7 In other words,
Wrist Extension on Table, From Armamentarium
Chirurgicum,
By Johannes Scultetus (1665)
by pulling on the hand, the bones will fall back in line on their own. Fellow sea surgeon Moyle essentially agrees, adding a bit of work for the surgeon. "[T]here must be two persons besides your self, who must make this extention, and in their extending wriggle the ...Hand and with your [the surgeon's] Hands at the Joynt your self must guide the [dislocated] bone aright"8.
Handley and Paré suggest a slightly different method, which Handley notes can be used for either a forward or backward dislocation. He explains the procedure thus: "the Hand must be laid upon some Table, with the back downwards, if the Dislocation be forwards; and if it be backwards, the contrary; then let good Extension be made, and with your Hand force the Bone into its place."9 Paré gives a slightly more graphic account, suggesting "the prominencies of the bones must be pressed down by the hand of the Surgeon, untill by the force of compression and site the luxated bones be thrust and forced into their places and cavities."10 Here the table is used to keep the non-luxed wrist bones in place while the out-of-place bone is pushed back into its proper position.
Sea surgeon John Woodall alone mentions the use of a device to extend the wrist.11 As with every other dislocation, he recommends the use of his Commander, although doesn't explain how it would be done.
Once the out-of-place bones were relocated, the wrist was medicated. Moyle suggests that the surgeon "embrocate with Ol Rosar. [Oil of Roses] and apply the defensive Plaster [to protect it from the air and unwanted humors]"12. If the surgical authors were tired of recommending medicines for a dislocated elbow, they seem to have just given up when they got to the wrist. The only other author to mention medicines is Atkins who says the surgeon "need not neglect Topicks [topical medicines] afore-prescribed"13, referring to those discussed previously in the standard dislocation treatment plan.
Atkins reports that this dislocation is "subject in its Consequence to great Pain and Tumor", noting that "Pain is a necessary Result from the greater Sensibility of the Number of Tendons here... [and] these large soft inflated Tumors, [are] the constant Attendant of Sprains and Distortions."14 To help prevent them, Atkins says proper bandaging is 
Dressings for Luxated Wrist, From A
Description of Bandages and Dressings,
By Charles Gabriel Le Clerc, p. 46 (1701)
important because the tumor results from an accumulation of blood and a "straight [tight] Bandage is most advantageously used"15 to prevent the blood from gathering there.
Charles Gabriel Le Clerc presents a bandage for a dislocated wrist in his usual fashion, with everything numbered and connected by a string as seen at left. He begins with a roller bandage (1), which is about an inch and a half wide and around nine feet long. Le Clerc specifies that the roller is to make "three Rounds about the Dislocation; bring the Roller over the Root of the Thumb, and then between the Thumb and Fore-Finger; bring it round the Thumb, to make an X about the bottom of it; descend over the Wrist"16. This will not use the entire roller. Le Clerc next applies a pair of pasteboard splints (2) dipped in oxycrate (water and vinegar) which "must be big enough to encompass the Arm, without touching it; they must be near six Inches long, and shaped round at the ends."17 They are to be wrapped with the remaining roller bandage until they are completely covered with cloth. The next dressing (3) is a 'small 'Pellet or Ball of Cloth, for the inside of the Patient's Hand, to keep his Fingers in a middle Posture"18. Once placed there, the rest of the roller bandage is wrapped over the hand and ball and back up the arm, ending by being wrapped around the elbow several times. The last dressing (4) is a piece of cloth which he calls a napkin used to make a sling to hold the arm.
There are only a few comments on long-term care of a dislocated wrist. Moyle advises the surgeon to "let the Man rest, and not stir that part too much"19. (Le Clerc's large bandage and sling would help certainly ensure limited movement.) Atkins suggests giving the wrist a cold bath and rest.20
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 398; 2 John Atkins, The Navy Surgeon, 1742, p. 113; 3,4 James Handley, Colloquia Chyrurgica, 1705, p. 158; 5 Paré, p. 397; 6,7 Atkins, p. 113; 8 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 125; 9 Handley, p. 159; 10 Paré, p. 398; 11 John Woodall, the surgions mate, 1617, p. 155; 12 Moyle, p. 125; 13,14,15 Atkins, p. 113; 16,17,18 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 46; 20 Atkins, p. 113
Specific Dislocation/Luxation Cure: Fingers
Treatment of dislocated fingers is discussed by four surgeons, but their comments are unusually brief. The fingers "may be dislocated, at least, distorted any way, backward, forward, or sideways"1. Richard Wiseman says the signs of such a dislocation "may be demonstrated by their Protuberance,

Photo: M. Dumont - Dislocated Thumb
and by the complaint of the Patient."2 John Atkins adds that "the Disparity is easily seen and felt."3
Both Wiseman and Atkins simply say extending [basically pulling] the finger will repair a dislocated finger, with Wiseman adding that the extension should be 'moderate'.4 Sea surgeon James Handley and Ambroise Paré advise laying the finger on a table to restore it.5 Paré's description is most informative: "they must bee laid straight upon a table, and so put into joint again. For thus they may bee easily restored, by reason their sockets are not deep, and their joints are shorter, and ligaments less strong."6 Handley adds that the surgeon should put "some hard Substance" under the hand when extending the fingers7, although it is not clear how this would help.
No one specifies a particular medicine for the fingers once they are repaired. Wiseman advises applying a common restrictive medicine8, Atkins suggests embrocations and plasters9 and Handley recommends 'fit' medicines.10 Presumably the surgeon would resort to those suggested in the standard dislocation treatment plan.
They are similarly vague about bandaging. Wiseman simply mentions using a bandage; Handley and Atkins suggest roller bandages.11 Fortunately, Charles Gabriel Le Clerc offers a description of dressings for dislocations of the finger.
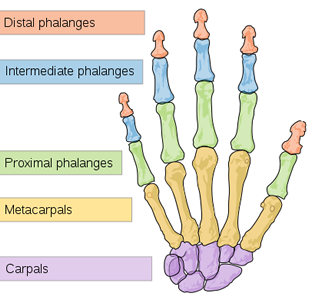
Image: Mariana Ruiz Villarreal - Bones of the Hand
He uses a modified version of his spica bandage for dislocations of the proximal phalanges. (The spica was described in the section on shoulder dislocations.) A small roller bandage is wrapped twice around the wrist and then wrapped up the hand to the site of the dislocation. "[M]ake an X on the Joint, descend with the Roller over the Wrist, to bring it up over the first Cast or Turn, and so [go back up to] make a second X on the Joint"12. This procedure of descending to the wrist and ascending back to the dislocation is repeated "till your Roller be almost spent, and then with the remaining Part, make Rounds about the Wrist to fasten the whole."13 The arm is then to be placed in a sling.
For the intermediate and distal phalange dislocations, Le Clerc again uses a small roller bandage, noting that the patient must keep his hand open while being bandaged. He starts at the wrist, wrapping it twice and ascends the hand to the site of dislocation. Then, "turn the Roller circularly round the luxated Part, descend insensibly the whole length of the Finger, by very small edgings, and end all with several Rounds about the Wrist and thus you will have a firm and secure Bandage, and the Patient cannot bend his Finger "14. He notably says that such dislocations "seldom happen, and I do not know whether they are possible"15.
Once medicated and bandaged, rest is recommended for long term care. The point of Le Clerc's bandage is clearly to immobilize the joint. Atkins advises 'repose'16. Fortunately, they heal faster than most dislocations; according to Paré the patient will recover strength in the joint in about twelve days.17
1 John Atkins, The Navy Surgeon, 1742, p. 116; 2 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 494; 3 Atkins, p. 116; 4 Atkins, p. 116 & Wiseman, p. 494; 5 James Handley, Colloquia Chyrurgica, 1705, p. 159 & Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 389 (mispaginated); 6 Paré, p. 389 (mispaginated); 7 Handley, p. 159; 8 Wiseman, p. 494; 9 Atkins, p. 116; 10 Handley, p. 159; 11 Wiseman, p. 494, Atkins, p. 116 & Handley, p. 159; 12,13,14 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 46; 15 Le Clerc, p. 46-7; 16 Atkins, p. 116; 17 Paré, p. 389 (mispaginated)
Specific Dislocation/Luxation Cure: Ribs
Sea surgeon John Atkins notes that they "are by their Closeness, a Security to one another against Injuries", but that they are still sometimes luxated. French surgeon Ambroise Paré says that the ribs "may by a great and bruising stroak bee dislocated, and fall from the
Artist: Andrew Bell - Sternum and Right Rib Cage
vertebræ whereto they are articulated, and they may be driven inwards, or sidewaies"2. Atkins only discusses ribs dislocated inwards or outwards. While it is difficult to see how a rib could be dislocated at all, let alone outwards, both sea surgeons Atkins and John Moyle discuss it.
When a rib is pushed inward, Atkins says "there follows great Pain, Cough, and Difficulty of Breathing"3. Paré adds "a painfulness in bowing down, or lifting up the body" to the list of symptoms.4 Atkins notes that the symptoms in an outward dislocation are not as bad. Paré finishes his introductory remarks about rib dislocations noting that unwanted humors will be generated at the site of a luxated rib and "the dislocation must be forthwith restored" to prevent them.5
For inward dislocations, both Paré and Atkins agree that there is little surgically to be done so the problem must "be remedied chiefly by internal Prescriptions."6 Neither suggests what medicines might be helpful in this situation, although those found in the discussion of Non-Penetrating Wounds of the Thorax would seem to be appropriate.
Sea surgeon John Moyle gives a straightforward description of the physical restoration of a dislocated rib: "you must lay the Patient on the well [uninjured] side over some round Substance as the Bilge of a Cask, or a Gun [cannon] (his clothes being off) and let your Assistant bend his body downwards and so will extension be made, that so with your hands you may place the ends of the Rib together."7 Atkins suggestion is even simpler, advising the the rib is easily returned "by an Elevation of the Arm, and pressing at the Proturbance with the Fingers at the same time"8.
Moyle offers a second method for relocating a luxated rib to be used when his first method doesn't work.
Lay on the Part the Stitch Plaster, made of Mastich, Gypsum, Terib. [turpentine] and aviarum Gluten [an animal glue made from the collagen found in birds] mixed, sowing Tape [woven fabric tape] to the outside of it to haule by when you have occasion; and when it hath lain on long enough so as to stick fast, then lay the Man in the posture as before, and hale up forcibly by the strings and the Rib will come into his Place."9

Fixing a Dislocation Over a Door, From Opera
Ambrosii, By Ambroise Paré (1594)
Since he is the only surgeon to mention a rib falling to the side (basically up or down), Paré gives the only description of restoring such a dislocation. If it is luxated up, "the Patient shall be set upright, hanging by his arms upon the top of some high door or window: then the head of the rib, where it stands forth, shall be pressed down untill it be put into its cavity."10 If it is luxated down, the surgeon must have "the Patient bend his face downwards, setting his hands upon his knees; then the dislocation may be restored by pressing or thrusting in the knot or bunch which stands forth."11
The big problem with a dislocated rib doesn't seem to be in replacing it, it seems to be in trying to keep it there. Atkins says that doing so "will not be altogether so easy."12 Moyle suggests first medicating the repaired luxation with oil of roses and his personal medicine for dislocations - defensivum minor.13
Atkins is a bit more glib, although he recommends a similar type of medicine. "The best Method that appears to me, is to keep your Hand upon the Defensative, (supposed to be apply’d,) until your Patient is laid in Bed."14 Once in bed he says "a Pillow should be placed in the room of it [in place of the surgeon's hand], to compress smoothly; and leave him to that fixed and quiet Posture the Pain makes him embrace."15 The purposes of a defensive medicine is to prevent air from reaching a wounded site.
Moyle recommends "decent Rouling: and at last Emplast. Catagmatic."16 The catagmaticum plaster was believed to build muscle, heat the area it was placed on and restrict the flow of humors to that part. Atkins disagrees, explaining that a roller bandage "increases both Pain and Difficulty of Breathing; however useful a just Straitness [tightness] is, in other luxated Joints, its not to be obtained here; slacking of Necessity, and not answering the End."17
Atkins makes no other suggestions for longer-term post-operative care other than putting the patient to bed on a pillow. Moyle recommends a couple of humoral treatments including letting blood "for this is absolutely convenient" and sweating him "to hinder the Coagulation of the Blood"18 He also advises giving the patient "Spruce Beer or the other Traumatic’s...to... heal inwardly... and let him have the fresh and wholsome Diet."19 However, Atkins dourly notes near the end of his commentary, "upon the Whole, reducing a Rib is little more than Formality"20.
1 John Atkins, The Navy Surgeon, 1742, p. 97; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 388 (mispaginated); 3 Atkins, p. 97; 4,5 Paré, p. 388 (mispaginated); 7 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 102; 8 Atkins, p. 97; 9 Moyle, p. 102-3; 10,11 Paré, p. 388 (mispaginated); 12 Atkins, p. 97; 13 Moyle, p. 103; 14,15 Atkins, p. 97; 16 Moyle, p. 103; 17 Atkins, p. 97; 18,19 Moyle, p. 103; 20 Atkins, p. 97-8
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-