

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 7
Specific Dislocation/Luxation Cure: Shoulder
Artist: Hans Holbien the Younger - Sailors at Work (1532-3)
All of the six surgical authors discuss luxations of the shoulder in some degree, indicating how relevant it was to sea surgeons and how likely it was to occur. Sea surgeon John Atkins points out that the shoulder is "more subject to Luxation than any other Joint, slight Accidents or Blows or Falls, frequently occasioning it."1 French surgeon Ambroise Paré adds that this is "because the ligaments of its dearticulation are soft and loose; as also for that the cavity of the shoulder-blade is not very deep; and besides, it is every where smooth and polite"2.
English military surgeon Richard Wiseman says shoulders are primarily caused by external forces. This is generally caused "by some violent force, either in Wrastling, Running, or by a Fall from a Horse, or the like. In the time of War it may happen by the force of great Shot or Splinters."3 He also notes that the shoulder luxation can be created internally by a "Fluxion [flow] of Humours upon the Muscles or Tendons, which gradually relaxeth them to such a degree, that the head of the Os humeri [humerus or upper arm bone] slideth down into the Axilla [armpit]."4 However, internally caused luxations are not discussed by any of the sea surgeons so were probably not common on ships.
When a shoulder is dislocated downward Moyle says, "You will feel the head of the bone [the humerus] under the Arm-pit"5. Wiseman agrees, adding that there will be "an unusual Cavity in the head of the Scapula, where it naturally is full and round ...the Patient's
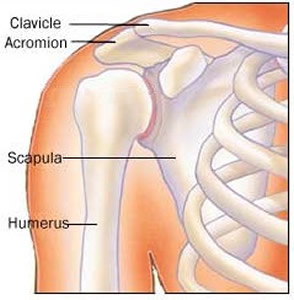
Image: AidMyRotaterCuff.com - Bones of the Shoulder
Elbow hangs from his Side, and cannot be brought so close as the sound without great Pain, nor can he bring his Hand to his Mouth, or stretch it upright against a Wall."6 Atkins notes that the Arm of the luxated shoulder will appear longer than the arm on the other side.7 Paré says "the acromion of the [shoulder] Blade shewes more sharp and standing forth than ordinary, for that the head of the shoulder-bone is slipt downe, and hid under the arm-pit, causing a swelling forth in that place; the Elbow also casts it self (as it were) outwards, and stands further off from the ribs; and though you force it, yet can you not make it to touch them."8
Everyone who discusses it agrees the shoulder can be dislocated in four different directions: "upwards, down-wards, or into the arm-pit, forwards and outwards, but never backwards, or to the hind part."9 However, Atkins points out, "It is almost ever dislocated downwards, rarely forwards, very rarely backward, or upward; the latter two Ways, I believe, have been added rather from the Possibility of the Thing, than Experience and Fact; for it is not easy to convince what Sort of Violence it must be, which can effect them"10. Since the methods discussed for fixing a dislocated shoulder by sea surgeons John Moyle and John Woodall are for one dislocated downward, the other types of dislocation will not be discussed in this article.11
Of the six authors who discuss the techniques necessary to restore a luxated shoulder, sea surgeon Hugh Ryder has the least of interest to say. He provides a case study which includes a luxated shoulder, but is focused more on other wounds that accompanied the dislocation.12 Wiseman, Atkins and Paré have the most to say on methods for repairing a dislocated shoulder, with Paré giving the most extensive explanations. Sea surgeons John Moyle, always direct, only mentions a couple ways to reduce a dislocated shoulder. John Woodall focuses mainly on the use of his device - the Commander - when extending the joint.
1 John Atkins, The Navy Surgeon, 1742, p. 102; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 388; 3,4 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 486; 5 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 122; 6 Wiseman, p. 486; 7 Atkins, p. 102; 8 Paré, p. 389; 9 Paré, P. 368; 10 Atkins, p. 102; 11 Those interested in the other methods are referred to Paré's book. He discusses forward shoulder dislocations on page 394 and outward and upwards dislocations on page 395; 12 For those interested in this case study, see Hugh Ryder, New Practical Observations in Surgery Containing Divers Remarkable Cases and Cures, 1685, p. 10-3
Extending and Replacing a Downwardly Dislocated Shoulder

Photo: Benutzer Hellerhoff - X-Ray of a Shoulder Dislocated Downwards
A wide variety of methods are discussed by the five surgeons who give detail on extending a patient's shoulder so that the downwardly dislocated humerus can be put back into its socket. These can be broadly divided into two categories: 1. Extensions by hand or with simple devices such as a band or a ball and 2. Extensions which employ more complex devices.
We first examine the hand-based methods and those which use simple devices and then examine the use of the more complex devices to restore a dislocated shoulder..
1. Extending and Replacing a Downwardly Dislocated Shoulder - Using the Hands and Simple Devices
The authors under study mention six simple ways of extending the shoulder: 1. Using the Hands, 2. Using the Knee and Thigh, 3. Using the Patient's Elbow, 4. Draping the Patient Over Other Men, 5. Using the Heel and 6. Using a Band with the Patient Upright.
Simple Shoulder Extension and Reduction Method 1 - Using the Hands

Surgeon and Assistants Working on a Soldier's Arm,
From Der
Vollkommene Teutsche Soldat,
By Hannss-Friedrich von Fleming (1726)
Richard Wiseman starts with the simplest method for restoring a dislocated shoulder. He notes that this is done by moving the bone "in a motion contrary to that it went out by."1 Ambroise Paré adds more helpful details:
First, let one [of you assistants] of sufficient strength, placed on the opposite side [of the patient], firmly hold the Patient upon the joint of the Shoulder, lest he move up and down with his whole body, at the necessary extension, working and putting it in: then let another [assistant], taking hold of his [the patient's] arm above the elbow, so draw and extend it downwards, that the head thereof may be set just against its cavity [socket] , hollowed in the [shoulder] blade-bone. Then at last let the Surgeon lift and force up with his fist the head of the bone into its cavity.2
Paré indicates that once the head of bone is freed and aligned, it will practically return itself to the proper position.
James Handley's suggestion is to use what he calls circumrotation. Here "you or the Patient puts the fist doubled under the Arm pit, so that the middle Knuckles, may force the [Humerus] Bone into its place, whilst with your other Hand, you make moderate extension [by pulling down], and keep the bone in a circular motion."3
While using only hands is the simplest method, it is also the most difficult to perform. Wiseman, Paré and Handley suggest it can only be used with young or less muscular patients. Even so, sea surgeon John Atkins says "the Hands, in my Opinion, are preferable to all these [other methods]; and have been sufficient with me, for reducing a Shoulder, even when the Head of the Bone, has been prolapsed three Weeks."4
Simple Shoulder Extension and Reduction Method 2 - Using the Knee and Thigh
Adjusting Using Head and Knees,
From Armamentarium Chirurgicum,
Johannes Scultetus, p. 52 (1665)
Richard Wiseman says that if one person is attempting to correct a dislocated shoulder he must rely on more than just his hands.
The knee and thigh method begins by seating the patient on a low stool and then having the surgeon place "his Fingers under his Arm-pit, his Knee or Thighs to the out-side of his Elbow, and his Head to the point of his Shoulder. By his Fingers strongly bent together, he pulleth the Bone both forward and upward. By his Thigh or Knee pressing his Elbow to his Side, he doth likewise help to raise it and bring it forward."5 Naval surgeon James Handley also suggests this method, although he recommends that "some stander by, press the Patient's Elbow (with the Knee) towards his Ribs."6
Wiseman admits it is a bit challenging, particularly on small men. His description makes it sounds like a contortionist's move. However, an image that very likely represents this method is shown in German surgeon Johannes Scultetus' book (at left) which doesn't make it look quite as complicated Wiseman made it sound.
Simple Shoulder Extension and Reduction Method 3 - Using the Patient's Elbow
Adjusting With Elbow,
From Der
Vollkommene Teutsche Soldat,
By von Fleming (1726)
The third method for fixing a shoulder luxation is quite simple, primarily involving the movement of the patient's elbow behind his back. There are two different ways mentioned for repositioning the dislocated shoulder this way.
Sea surgeon John Moyle explains the first method quite simply. He says it is performed "by your taking the Patients Hand, and putting it behind in his Neck, with one [assistant] to hold it there, and then you with your hands forcing suddenly at his Elbow, and withal bringing it close to his Breast, the bone will locate."7
Richard Wiseman suggests a second method, which involves bringing the patient's elbow behind him where it is "held close to the Spine, whilst the Chirurgeon presseth with both his Hands forcibly upon the head of the Bone [in the patient's armpit to move it back up into its socket]."8 Although similar to the Method Moyle uses, Wiseman's suggestion is a little more complicated because the surgeon is actually involved in trying to place the humerus back into its socket with his fingers.
Simple Shoulder Extension and Reduction Method 4 - Draping the Patient Over Other Men

Draping the Patient Over Others, From The Workes of
that
Famous Chirurgion
Ambrose
Parey, p. 390 (1649)
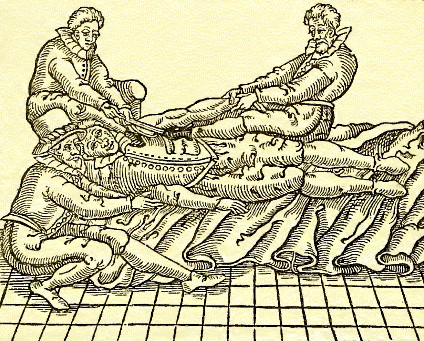
Another way to reduce the luxated shoulder is by draping the patient over other mens' shoulders. Ambroise Paré says that this "is most fit for new and easily to be restored luxations" along with Method 1.9 He recommends having an assistant who is "of a competent height and strength" put "the sharp part of the top of his shoulder under the Patients arm-pit"10. Wiseman describes this part a bit differently recommending "a proper lusty Fellow on whose shoulder you must hang the Patient by the luxated Arm, bringing his Hand over to the Fellow's Breast."11
Paré then says the patient "shall somewhat violently draw his arme towards his owne breast, so that the Patients whole body may (as it were) hang thereby."12 Wiseman suggests that when "the weight of the Patient be not sufficient to make the Extension, some other body [person] may hang upon him, or pull him by the Legs downward."13 With a similar idea, Paré recommends "for the greater impression, [another assistant] shall lay his weight on the luxated shoulder" who will move and shake the arm while pulling it down.14 He also notes that surgeon is to help "with his hand governing these violent motions, as this figure shews [at left]."15 Although neither Wiseman nor Paré mention it, John Atkins points out that this is basically the same way the humerus is relocated using a ladder.
Simple Shoulder Extension and Reduction Method 5 - Using the Heel
The fifth simple method to extend a dislocated shoulder uses the heel of the surgeon or an assistant to push the
Fixing a Dislocated Shoulder Using the Heel, From The Workes of that
Famous
Chirurgion
Ambrose
Parey, p. 390 (1649)
bone back into place. Ambroise Paré says the patient must be laid on his back on a mat with a large, soft ball stuffed into his armpit in preparation for this procedure. The surgeon is to sit next to the patient right up against the dislocated shoulder. "[I]f his right shoulder be luxated, he [the surgeon] shall put his right heel to the ball, which filled up the arm-pit; but if the left, then the left heel: then let him forthwith draw towards him the Patients arm, taking hold thereof with both his hands, and at the same instant of time strongly press the arm-pit with his heel."16 At the same time, an assistant is to "lift up his shoulder with a towel, or some such thing fitted for that purpose, and also with his heel press down the top of the shoulder-blade: another also shal sit on the other side of the Patient, who, holding him... at the necessary extension in setting it"17.
Sea surgeon John Atkins and Richard Wiseman also describe this procedure without adding much to Paré's vivid description. Atkins does not view the method very favorably, noting that "the Posture is incommodious for Reduction"18. He further explains that the surgeon or assistant pulling the patient's arm down is wasting some of his effort because "the Elbow-Joint interposing, abates the force of the Extension."19 Even Paré recommends this procedure primarily for patients who unable to sit or stand, suggesting the methods which involve the patient being upright are better suited to relocation.
Simple Shoulder Extension and Reduction Method 6 - Using a Band with the Patient Upright
The sixth simple method to extend a dislocated shoulder involves using a band. Both Atkins and Wiseman advise using belts only on strong, muscular patients where extra force is required. Wiseman recommends using a girt, which "hath a Boulster [a piece of cloth folded several times] in the middle, and the ends are tackt firmly together."20 Atkins specifies the use of a Napkin, which is basically a piece of rectangular cloth. He says that it is "to sit broad [presumably, not folded so it is comfortable and provides even force] on the Hurt-side, the upper Edge of it to come close to the

Extending the Shoulder of an Upright Patient with a Band,
From From Armamentarium Chirurgicum, By
Johannes
Scultetus, p. 52 (1665)
Axilla [armpit] and on the opposite Part to be tied very fast"21. The end which is tied is to be pulled by an assistant. The actual extension and reduction methods using bands employed by Wiseman and Atkins are slightly different although the result is similar. Let's look at each in turn.
Wiseman says the boulster on his girt is to be placed in the patient's armpit and the other side around the surgeon's neck, "that he may thereby with all his force raise up the head of the Humeris"22. Although he does not specify it, the patient must be seated on a low stool in order for the surgeon to position himself properly. The surgeon's assistant is to sit behind the patient, "and pull his [the patient's] Arm backward with all his might; and if the Chirurgeon presseth with his Hands upon the head of the Scapula at the same time he raiseth up the Humeris, he shall reduce it more easily."23 Here again we have Wiseman putting the surgeon into a contorted position to extend the luxated joint. The point of the band is clearly to supplement the force applied to the bone by the surgeon's hands.
In Atkins' method, the patient is seated on a low stool with room around him for the surgeon and his assistants to help without getting in each other's way. Extension is made by pulling the humerus down. This is performed by someone who is "strong, and [who will] have his Hands flowered [covered with flour], for the more firm holding"24. At the same time, contra-extension is performed by someone pulling upwards on the band which is wrapped around the Patient's shoulder "Extension and Contra-Extension should be begun together, not by Jirks, but smooth, steady and strong" 25 While this is happening, the surgeon is to place "his Thumbs forcibly on the Cervix of the Scapula [on the top of it near the acromion], and his fingers underneath in the Axilla [armpit], without any Linnen or Compress between to dull the Sense of Feeling, when the Head of the prolapsed Bone is moving."26 He is to use "all the Strength he has in his Fingers, to assist its Reposition, ordering him that extends, to favour this Part, by moving the Elbow downwards towards the Patient’s Side, when he is at the full Stretch of it."27
1 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 487; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 389; 3 James Handley, Colloquia Chyrurgica, 1705, p. 156; 4 John Atkins, The Navy Surgeon, 1742, p. 103; 5 Wiseman, p. 487; 6 Handley, p. 156; 7 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 122; 7 Wiseman, p. 487; 8 Paré, p. 389; 9 Paré, p. 390; 10 Wiseman, p. 487; 12 Paré, p. 390; 11 Wiseman, p. 487; 14,15,16,17 Paré, p. 390; 18,19 Atkins, p. 103; 20 Wiseman, p. 487; 21 Atkins, p. 103; 22 Wiseman, p. 487-8; 23 Wiseman, p. 488; 24 Atkins, p. 103; 23 Atkins, p. 104; 26 Atkins, p. 103; 27 Atkins, p. 104
2. Extending and Replacing a Downwardly Dislocated Shoulder - Using Complex Devices
In addition to the simple methods, the authors under study examined seven complex devices which could be used to extend a luxated shoulder. The mechanics of these devices have already been discussed in the section Devices for Extending Dislocations/Luxation, so those will not be mentioned in detail. Links to each device's description are included for those wishing to review their function. The complex methods for extending a shoulder include: 1. The Ladder, 2. The Coulstaff, Poles and Doors, 3. The Crutch, 4. The Ambi, 5. Pulleys, 6. The Glossocomium and 7. The Commander
Complex Device 1: The ladder functions in about the same way as the simple method of draping the patient over other men discussed previously, placing the unseated humerus bone on a soft ball on the rung of the ladder and then either dropping the patient onto the rung or having men hang on him to force the bone back into its socket.
Using a Board on a Dislocated Shoulder - This is the
Basic Principle Behind Methods 1-3,
From
Armamentarium Chirurgicum, By
Johannes
Scultetus, p. 46 (1665)
It is discussed by Richard Wiseman1, sea surgeon John Atkins2 and Ambroise Paré3. It is primarily used by these authors for dislocated shoulders, the method for which is discussed in detail on the device page.
Complex Method 2: The second complex type of device includes the coulstaff, poles and doors. Such things are to be placed with a pad or ball under the patient's armpit and then the device is either lifted by two men or, when the device is stationary, the patient is to fall on them, forcing the humerus back into the shoulder socket. Poles and doors are suggested as substitutes for the actual coulstaff by some of the period authors. The coulstaff and variations of it are mentioned for use with luxated shoulders in the texts of John Moyle4, Richard Wiseman5 and Ambroise Paré6.
For the most part, this method functions in much the same way as the ladder does and was discussed in detail previously. However, John Moyle adds a detail when using it on a patient's shoulder which wasn't mentioned previously. He advised that before attempting to restore a joint in this manner, the surgeon should "anoint the Joynt well with Ol. Rosarum [oil of roses]"7. None of the other surgeons suggest this and Moyle doesn't explain why he chooses to do so. However, physician Nicholas Culpeper suggests that oil of roses was useful for reducing swellings and inflammations8, which likely has something to do with Moyle's recommendation.
Complex Method 3: The crutch is suggested exclusively here by sea surgeon John Atkins9. Based on his description, it is a pole that is fastened to the floor with a knob or ball on top which is placed in the armpit of the Patient. Properly positioned by the surgeon, the patient drops onto the ball and it forces the humerus back into place. This is once again very similar to the ladder method.
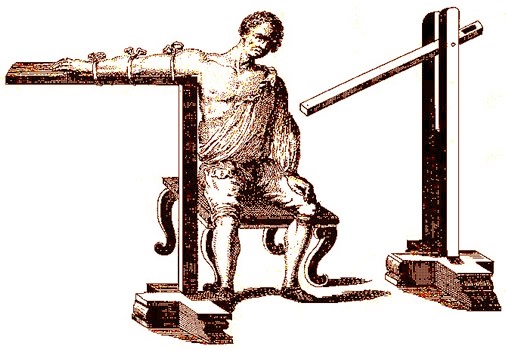
The Ambi, Show With and Without a Patient, From A General System of Surgery, By Lorenz
Heister, Plate 10 (1750)
Complex Method 4: The Ambi was a device created specifically for reducing dislocated shoulders. It is mentioned by surgeons John Atkins10 and Ambroise Paré11. It works somewhat differently than the previous three devices in that it has the patient stick his arm out parallel to the ground on a board with a ball at the end which is shoved into the armpit so that it rests under the unseated humerus. The board pivots on a stand, which allows the surgeon to pull down on it and push the ball into the humerus and force the bone back into its socket. This can be seen in the diagram at left. A fuller description of the ambi appears on the devices page with each part lettered and their function being described in detail in the accompanying text.
Paré's Pulley in Use, From The Workes of that Famous Chirurgion Ambrose Parey (1649)
Complex Method 5: Ambroise Paré presented an image of a device containing six pulleys which were used to dramatically increase the amount of force an individual could apply to a luxated joint. The pulley is attached on one end to a cord which is tied to the limb being pulled away from the joint and on the other end to an eye screw which is turned into a solid object such as a post, wall or floor. By pulling on the rope that feeds through the device's pulley system, the joint can be very forcefully extended.
The pulley has a large amount of support among the surgeons under study for extending a dislocated shoulder, being suggested by Richard Wiseman12, sea surgeons John Moyle13, John Atkins14 and James Handley15, and Paré himself16. The ever practical Moyle's praise for this device as being the best available for shoulder luxations suggests its usefulness to surgeons serving on ships.
Complex Method 6: The Glossocomium is mentioned by several authors in relation to extending a dislocated shoulder, however none of them favor it. Paré suggests that his pulley would be a better device for this purpose.17 In fact, the pulley would serve the same basic function as the glossocomium and take up far less space, something that would be of great concern to a ship's surgeon.
Complex Method 7: The last device suggested for extending a shoulder was John Woodall's Commander. Woodall is the only author under study to discuss this device.18 Since he does not provide an image of it and his description is wandering and vague, its exact configuration is not entirely clear. However, it appears to function in a manner similar to the Glossocomium when extending a luxated bone and to the ambi when pushing the end of the humerus back into place.
1 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 488; 2 John Atkins, The Navy Surgeon, 1742, p. 104; 3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 391-2; 4 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 121-2; 4 Wiseman, p. 488; 6 Paré, p. 391; 7 Moyle, p. 121; 8 Nicholas Culpeper, Pharmacopœia Londinesis, 1720, p. 218; 10 Atkins, p. 104; 11 Paré, p. 391; 12 Wiseman, p. 488; 13 Moyle, p. 122; 14 Atkins, p. 104; 15 James Handley, Colloquia Chyrurgica, 1705, p. 156; 16,17 Paré, p. 389; 18 See John Woodall, the surgions mate, 1639, p. 155-6
Securing a Downwardly Dislocated Shoulder and Post-Operative Care
John Atkins explained that the surgeon could tell that the dislocation was restored when "the Joint and Arm recovers a Similtude with the sound one,
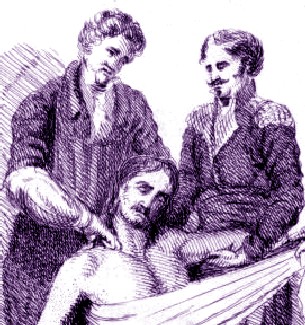
Working on the Patient's Shoulder, From Chirurgie,
Medicins et Malades, By Charles Bell (1821)
Pain is abated, and what we may add, as a surer Sign than all, is the snapping Noise that will be heard at its returning into the Socket."1 Once the humerus had been put back into place, the dislocated shoulder was secured using medicines and bandaging.
For medicines, Ambroise Paré ordered the surgeon to "cover all the adjacent parts with a medicine made ex [from] farina volatili [mill dust], bolo armenio [Armenian earth], myrtillis [myrtles - possibly the berries], pice [pitch], resina [pine resin] & alumine [alum], beaten into powder, and mixed with the white of an eg."2 Sea surgeon John Moyle tells his readers to "embrocate well with Ol Rosar. [oil of roses] and apply Emplastrum defensivum minor ...about the Joynt"3. The defensive plaster is one of Moyle's own creations which he particularly recommends for use on dislocations. For adults, Atkins recommends embrocating the joint with a combination of equal parts of oil of lilies and oil of St. John's wort. He then recommends a variety of things discussed previously in the general treatment of luxations: a plaster containing several ingredients (Diapalma Plaster, Red Lead Plaster and Armenian earth), Emplaster é bolo or common wax - any of which he says can be used to "resist Pain and Influx of Humors."4
Next came bandaging. As usual, Moyle's comments were the simplest:
Arm in Sash, From Ministerium des Innern der DDR
"let a Bolster [folded lint bandage] be kept under the Arm-pit, and let him carry his Arm in a sash till ‘tis well."5 Paré expands greatly upon this. Like Moyle, he recommends a ball of yarn or a bolster be put into the armpit. The shoulder was then to be spread with oil of roses, oil of myrtle, a little vinegar and either rose unguent or cold cream. The medicines were most likely to encourage healing and prevent air from getting to the wound and corrupting the humors.
The shoulder was then to be bound with a roller bandage split in two at each end about four inches across and thirty-six inches long. "The midst thereof shall be put immediately under the arm-pit, and then crossed over the lame shoulder, and so crossing it as much as shall be fit, it shall be wrapped under the opposite arm. And lastly, the arm shall be laid upon the breast, and put in a scarf, in a middle figure almost to right angles, so that by lifting up the hand he may almost touch his sound shoulder"6.
Atkins then recommends one of two courses, depending on the patient's age. For young patients "of good Constitution, [there] need only be a Compress large enough to infold the Joint, dipped in Oxycrate [vinegar and water], or Acetum cum Albumine Ovorum [Vinegar with egg whites]"6. Older patients are to have it bandaged per Charles Gabriel Le Clerc's book which will be explained shortly. Once bandaged, "The Situation of the Limb should be in a large Napkin, thus: Bring one Edge of it close under the hurt Joint; carry one Part behind, the other forward, and tie fast on the opposite Side of the Neck; the inferior Selvedge [a woven band on the edge] of the Napkin bring up, having inclosed the Cubit, and pin at a suitable Elevation."7
Shoulder Luxation Dressings, From A
Description of Bandages and Dressings,
By Charles Gabriel Le Clerc (1701)
Le Clerc's dressings have their usual detail and accompanying diagram, showing each individual component numbered and connected by a string.
The first dressing element (1) is the piece put under the patient's arm which Le Clerc refers to as a 'small Pellet of Linnen". It is there to keep the head of the humerus in place. He refers to dressing element 2 as a 'Sling with four Tails' which is used to keep the pellet of linen in place in the patient's armpit. "The undivided part of the Sling is to be applied on the Pellet, and the four Tails raised on the Shoulder, where they must be crossed and fastned with Pins."8 On top of all this is placed the element 3: "A Compress of Linnen, in several Doubles, to be put under the sound Armpit, to keep the
Bandage from galling it.”9
With the armpit well covered, the last element of Le Clerc's dressing is a bandage he calls the Spica.

A Spica-Like Shoulder Bandage
From
A General System of Surgery
By Lorenz Heister (1743)
He explains that this is made using a roller bandage (4) that is five ells, or about ninety inches long. This is started under the armpit of the non-dislocated arm and then going across the body and over the affected shoulder. Then it goes under the affected armpit and back across making an 'X'. This is done again with the next pass bringing the bandage closer to the patient's neck and continued until the surgeon nearly runs out of material. He is then to wrap it twice around the arm and pin it. Le Clerc adds, "If any one would make the Spica, he must make a great Number of X’s to cover the length of the Clavicle; and. to keep down every X very well, he must pin it in the Place where it crosses"10. Of the Spica bandage, Atkins says it "will be always best for the Shoulder; and... is usually dipped in Oxycrate, or Red Wine"11. Atkins also notes that the surgeon must "keep the Circumrotations tort [taut]; because, what with the drying of the Rowlers and Motion of the Breast in breathing, they soon slacken."12
Not much is said about post-operative care. Richard Wiseman advises that although the humerus can be restored to its proper place in a variety a ways, it "doth require your industry to retain it after it is reduced"13. Paré recommends that after the shoulder has been dressed the first time, it is shall not "be stirred, untill four or five dayes be past, unless the greatness of some happening symptome divert us from this our purpose."14 Time seems to be the key to the long-term healing of a dislocated shoulder.
1 John Atkins, The Navy Surgeon, 1742, p. 104; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 389-90; 3 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 122; 4 Atkins, p. 105; 5 Moyle, p. 122-3; 5,6 Atkins, p. 105; 7 Atkins, p. 106; 8,9 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 24; 10 Le Clerc, p. 22; 11,12 Atkins, p. 105; 13 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 488; 14 Paré, p. 390
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-