

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 8
Specific Dislocation/Luxation Cure: Elbow
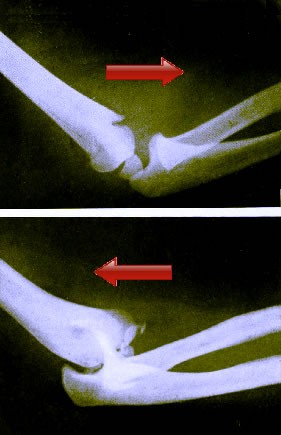
Top - Inward/Forward/Anterior Dislocated Elbow
Bottom: Outward/Backward/Posterior Elbow Dislocation.
From
Radiography
and Radio-Therapeutics,
By Robert Knox (1917)
Each of the four surgical authors who discuss dislocation of the elbow agree that it is possible to do so four different ways, the clearest description of which appears in the books of Richard Wiseman and sea surgeon John Atkins: inward, outward, and to each side1 However, Atkins points out that it is unlikely to be dislocated sideways based on the joint's "Make, and strong Ligaments on its Sides"2. In addition, Wiseman and sea surgeon John Handley do not discuss the correction of sideways dislocations of the elbow so the cure of sideways luxations will not not be discussed here.
Ambroise Paré goes to rather extraordinary lengths to explain what each type of dislocation was, although his explanation creates more confusion than clarity.3 However, Paré talks about inward and outward dislocations of the elbow in a way that suggest they are the same as the forward and backward dislocations of Wiseman, Atkins and Handley. To further confuse things, modern doctors abandoned these descriptions, describing simple elbow dislocations as anterior (aka. forward/outward) and posterior (aka. backward/inward). Of the three names, forward and backward are the most widely used in the period texts and the most descriptive, so that's what will be used in the rest of this section. For those curious what all these things actually refer to, see the image at left for a graphical representation of them.
Atkins says it is difficult to see how the elbow can be 'perfectly' or completely dislocated. Wiseman concurs, noting that "perfect Luxations of this Joint do rarely happen. When they do, they are difficultly restored"4. Paré agrees, noting that the elbow is harder to re-set than the shoulder and adds a warning that the elbow is "also more subject to inflammation, and to grow hard thereupon, as Hippocrates saith."5
Atkins points out that an backward luxation is the most likely. Paré explains that "if at any time the cubit [forearm] be bended more straitly and closely than that the inner process can retain its place and station in the bottom of its sinus [the cavities for the bottom of the humerus in the bones of the forearm] the hind process falleth out and is dislocated backwards."6

Examining the Elbow, From Armamentarium
Chirurgicum
Bipartitum, By Johannes Scultetus (1666).
A forward dislocation is less likely because a dislocated bone of the forearm (either the ulna or radius) must be "extended more violently [than a backward dislocation], and forced against the bottom of its cavity, it flyes and departs out of its place as beaten or forced thence, and this kind of luxation is far more difficultly restored than the former"7. Atkins suggests that this can be caused during high falls where "the Person endeavours to save himself with the Palm of his Hand; for then the Strain lies entirely at the Elbow, (the Wrist yielding, and the Pressure along the Cubit being secundum Longitudinem, [along the length]) so that if of Necessity something must give way, it will probably be here [at the elbow]"8.
Handley says the signs of a forward luxation are that "the Arm cannot be bent; the Cubit [forearm] is shorter; a Tumor appears on the fore-part, and a Cavity behind"9. In a backward dislocation, he simply says the signs are 'the contrary'.
Atkins doesn't talk about the different types of dislocation at all, simply explaining that dislocated elbows feature "a Protuberance [protrusion of the unseated bone] on which Side soever the Head of the Bone thrusts out, a Cavity [occurring in the place from] whence it has receded, and an uncommon Pain from a Distraction [pulling or tearing] of the Tendons, the Flexors, and Extensors of the Hands and Fingers"10.
Once an elbow dislocation has been diagnosed, Paré orders the surgeon to "forth with undertake the restitution thereof, for fear of defluxion [flows of unwanted humors] and inflammation, which the bitterness of pain usually causeth, upon what part soever the luxation happen."11
1 See John Atkins, The Navy Surgeon, 1742, p. 109 and Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 492; 2 Atkins, p. 109; 3 For the adventurous, see Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 395; 4 Wiseman, p. 492; 5,6,7 Paré, p. 395; 8 Atkins, p. 110; 9 James Handley, Colloquia Chyrurgica, 1705, p. 158; 10 Atkins, p. 110; 11 Paré, p. 396
Extending and Replacing a Dislocated Elbow
Sea surgeon John Atkins sums up the extension and replacement of a dislocated elbow very simply: "To reduce, is to extend and force the Head of the Bone contrary to the Way it Prolapsed."1 However, such a brief description probably wouldn't have been very helpful to a new surgeon who was relying on a book to guide him in putting a dislocated elbow back into place.
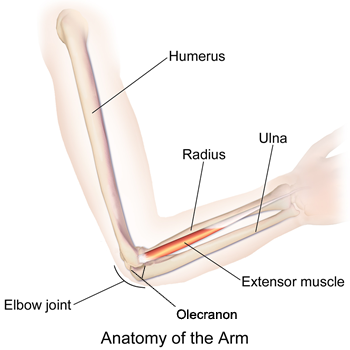
Image: Bruce Blaus - Anatomy of the Arm
The three other authors who discuss dislocations of the elbow present a variety of ideas for extending and replacing it. French surgeon Ambroise Paré provides separate descriptions of the procedures for both the forward and backward dislocation. Sea surgeon James Handley gives a detailed procedure for forward dislocations of the elbow, but only says that the backward dislocation "is to be reduced the contrary way"2. Wiseman's recommendation is similar although he notes that for a backward elbow dislocation "the extending [extensor] Muscles of the Cubit [forearm] are very strong, it will be necessary that the Muscles serving the Cubit be first well embrocated with lenient Ointments"3 to soften them and make extension easier. He doesn't specify which ointments, but a list can be found here.
There are essentially two methods for repairing an elbow dislocated forward: using the hands and using devices such as a ball, girt [belt or band] and/or post.
To relocate the radius and ulna by hand, an assistant holding the patient's arm just under his shoulder joint pushes it forward. The surgeon, must move the forearm of the dislocated shoulder inwards and "by little and little draw and extend the arm, wresting it gently this way and that way, that he may bring back the bone which fell out into its cavity."4

Although This Method is Not Discussed, The Concept is Similar
From Florentini Opera Varia, By Vidi Vidii, p. 493 (1599)
Handley warns the reader that this cannot be done unless the arm is held straight, because "whilst the arm is bended or crooked, the cubit [forearm] is only lifted up, and not drawn into its seat." Handley also mentions that the bone can be relocated by hand when a patient is young or when the elbow hasn't been dislocated for very long, but he doesn't provide any details on doing so.5
Wiseman suggests another hand-based technique for treating an outward dislocation. In his procedure the arm must be placed 'obliquely' (bent), "not in a straight line, lest you break the tip of the Ulna"6. This requires two assistants to extend and counter-extend the elbow. A third person "must guide the Elbow so as to keep it bent, and to direct the Bone"7 using a bolster to press down on the joint so that the bone can be put back into place.
For device-based methods, variations on extending and replacing an elbow dislocated forward are presented. From Handley: "[L]et a hard Body of Linnen (essentially functioning as a ball) be placed on the inside of the Joynt, and over that a Girt (belt) so long as that you may 
Extending a Forward Dislocated Elbow, From Ouvres, By
Ambrose
Paré, p. 480 (1575)
put your Foot into it; then whilst they make due Extension, (by your Foot in the Girt, and by your Hands) bend it, and reduce it"8. Stepping on the girt while the arm was crooked would pull the whole forearm down if the patient could keep it out straight, allowing the surgeon to slide it into place. Wiseman says that in this variation, the girt is to be pulled behind the elbow where it functions "in the nature of a Stirrup, in which the Chirurgeon may put his foot"9. Handley's description hints that one person could do this, something that could be useful to a lone sea surgeon when necessary.
Paré also recommends a device-based method where "the dislocated arm [is] lightly bended to embrace a poste, then must the end of the cubit called Olecranum [olecranon] be tyed or bound about with a strong ligature or line, and then wrested into its cavity by putting a battoon [baton] or staffe into the ligature"10. The ligature is used to pull the bone down and backward as seen in the image at left. Paré says the surgeon will know he is successful "when the pain ceaseth, and the figure and whole naturall conformation is restored to the arm, and the bending and extending thereof is easie, and not painfull."11
Paré is the only surgeon to give a procedure to repair a backward dislocation of the elbow. His procedure is simple: "the arme must bee strongly and powerfully extended [presumable by two assistants], then bended quickly and with sudden violence, so that his hand may smite upon his shoulder. Some put some round thing into the bought of the Elbow, and upon that doe suddenly force the Elbow to the shoulder, as wee have formerly said."12 This maneuver would presumably jerk the forearm forward and force the ulna and radius forward and back into their proper place.
1 John Atkins, The Navy Surgeon, 1742, p. 110; 2 James Handley, Colloquia Chyrurgica, 1705, p. 158; 3 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 492; 4 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 395; 5 Handley, p. 158; 6,7 Wiseman, o, 492; 8 Handley, p. 158; 9 Wiseman, p. 492; 10,11 Paré, p. 396; 12 Paré, p. 397
Securing the Elbow and Post-Operative Care
Once the bone(s) have been replaced,

Image: flagstaffotos.com.au - St. John's Wort Flowers (Hypericum perforatum)
the elbow was medicated and bandaged.
For medicines, Richard Wiseman simply says to use restrictives. These stop fluids from flowing and are often used to refer to styptic medicines. Here it more likely refers to medicines which prevent humors from flowing to the part, because he adds "these Luxations are subject to great Fluxion [flows of humors], Inflammation, &c."1 Ambroise Paré only suggests the use of "fit medicines formerly mentioned"2. (Clearly some of the surgical authors were getting tired of writing the same things over and over.) Sea surgeon James Handley also recommends restrictives, along with oil of roses and vinegar3. Sea surgeon John Atkins advises the use of emollients (softening medicines - possibly to relax the muscles and nerves) and anodines or pain-killers. He also specifies, "Embrocate with Ol. Hyper. [Oil of St. John's wort] Rosar. [Oil of Roses] a. p. ae [mixing equal parts of each]."4
For bandaging the elbow, Handley says "make decent Bandage, place the Arm in a middle Posture"5. Paré is also brief, advising
Dressings for Luxated Elbow, From A
Description of Bandages and Dressings,
By Charles Gabriel Le Clerc, p. 37 (1701)
the surgeon to "lay the arme in a straight angle, and so binde it up, and ... let him carry it in a scarfe put about his neck"6. After spending so little time explaining how to extend and reduce a luxated elbow, Atkins makes up for it in the description of bandaging it. Most of his comments follow the description given by Charles Gabriel Le Clerc from which they are likely taken, so his diagram will be used here with references to it inserted into Atkins' description.
...dip a double Flannel (snipped from each End toward the Middle) [1] into the same Mixture [oil of St. John's wort and Oil of Roses] warm, and apply: It is, I conceive, better than a Plaister, as being more soft and anodyne, and compliable to the Shape and Position we are to put it in. The Rowler [2] should be single [have only one head]: Begin, with one Turn on the lower End of the Os Humeri [humerus], slope it down on the Bending of the Arm, and make a Turn on the upper End of the Cubit [forearm], re-ascending on the Bending of the Arm, so as to make a Cross there; continue so to do with Edgings, till the Whole be covered, (except the Tip of the Elbow) and finish at the upper Part of the Arm. You must give the Cubit a little Flexure before Rowling; and the Elbow not being covered, will yield enough to sling [3] at a proper Elevation.7
Post-operative care includes bleeding and "a cooling Diet, and his Body [kept] soluble [loose and open]."8 Paré explains that a callus forms quickly in elbow luxations "by reason that by rest and cessation from the accustomed actions" which, combined with the pain the joint experiences causes an abnormal bodily humor to "floweth downe... [which] is hardned, and gleweth the bones together"9. Because of this, he says that the sling "must be loosed sooner and oftner than otherwise, that is to say, every third day, and then the Patients arme must be gently moved every way."10 Here we have the most basic form of physical therapy. If this is done, Paré says the patient should recover in twenty to twenty-five days.
1 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 492; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 397; 3 James Handley, Colloquia Chyrurgica, 1705, p. 158; 4 John Atkins, The Navy Surgeon, 1742, p. 110; 5 Handley, p. 159; 6 Paré, p. 397; 7 Atkins, p. 110-1; 8 Handley, p. 159; 9,10 Paré, p. 397
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-