

New World Quarantine Page Menu: 1 2 3 4 5 6 7 8 9 Next>>
New World Quarantine During the Golden Age of Piracy, Page 2
Purpose of Maritime Quarantine - Smallpox Description
“'Tis I know the common Opinion, that any Old Woman can cure the Small-Pox: For my part, I do profess I do not know any Distemper that requires more Care, and a Physician's Diligence and Skill.” (William Oliver, A Practical Essay on Fevers, 1704, p. 198-9)

Aztecs with Small Pox, Florentine Codex (16th century)
Of the illnesses which people tried to prevent using maritime quarantine in the late seventeenth and early eighteenth centuries, smallpox was one of the oldest and most deadly in terms of the sheer number of people who died. "By the turn of the eighteenth century, the disease had become endemic in the major cities of Europe and the British Isles. Nearly one-tenth of all mankind had been killed, crippled or disfigured by smallpox: ‘No man dared to count his children as his own until after they had the disease.’"1
Several attempts were made to quarantine ships which might bring this infectious disease into the North American colonies before and during the golden age of piracy making it an important part of maritime quarantine. Being employed primarily in the American Colonies, these quarantine systems were nowhere near as formal or organized as the system used in the Mediterranean to try to prevent the plague. Sailors were instead directed to remain aboard their vessels to serve out quarantine.
1 Michael B. A. Oldstone, Viruses, Plagues, and History, 2000, p. 35
Theory
When discussing the cause of smallpox, English physician William Oliver compared it to a seed of poison, which took three different forms. However, he then said, "What this Poyson is, or how it operates on our Constitutions, is too large a Field of Argument at this time, and therefore I shall pass it by, and only show how many Species we meet with of this Disease, and how they differ from each other."1 While mulling the reason diarrhea accompanied a virulent smallpox, physician Thomas Sydenham likewise backed away from the theory behind it, suggesting, "I only write a History, and do not pretend to solve [such] Problems."2
Artist: Pieter Phillipe
Dutch Physician Gideon Harvey (1663)
One physician who had a great deal to say about how smallpox functioned was Dutch physician Gideon Harvey. Not surprisingly, his theory centered on the transmission of the disease by air, the usual culprit for such inexplicable illnesses during this period. Harvey said that the 'half-pestilential' smallpox "Particles are more frequently floating in or about Cities, and Towns, it’s not very rare to meet with them in scattered Villages, arising out of Church-Yards, standing Pools, stinking Ditches, or Morasses, and places where Garbage Carrion, and other Nastiness is thrown, so that it’s sometime equally possible to fall into that Disease in the Country, as in Cities, or Towns."3 He further states that a 'half' or 'demi-pestilential' smallpox infected air reached its victims through their pores.
Harvey was not alone in this belief. Sea-surgeon Thomas Aubrey said that when infected air
enters the Body, it must of Necessity cause an inordinate Motion of the Humours [fluids], and procure Sickness, of which one may introduce a very terrible Instance, which is that of the Pestilence [plague], and (I believe I may be bold to say) also the Small-pox; which are both of them contagious Diseases, and seem to be procured by an evil malevolent Diathesis [condition] of the Air, vitiated [spoiled] by means of some certain malignant Vapours, that were confined within the Caverns of the Earth4
Aubrey goes on to explain that when the land is disturbed by things such as earthquakes, the earth's "Pores are dilated, and so give way for those venomous Vapours to rush forth; whence the circumambient [surrounding] Air, and consequently the Blood, and substantial Parts of their Bodies, who inhabit those Parts, are tainted"5.
Harvey says that a person must also have the right 'disposition' to contract smallpox. He lists

Artist: Julien Henri
Defeating The Dragon Smallpox (1876)
three elements which he says are necessary. The first element is the humors (fluids in the body) "whose Pores the insufficiency of [normal] Spirits being incapable of filling, are the readier enter’d and possest by the half pestiferous Particles."6 The second element is pores which are correctly configured to allow these particles to enter. The third element is "Feebleness and poverty of the Spirits; laxity of the ambient Membranes and Humors, besides several other Concurrents."7
Physician Thomas Sydenham discusses a more practical theory focused on how the body eliminated smallpox. He said that two operations occurred once the disease had found its way into a body: separation and expulsion. Separation occurred in the first three or four days, involving 'febrile Ebullition', essentially referring to boiling in the blood via fever, "in which time Nature is busied in gathering together the inflamed Particles which molest the Blood, and in thrusting them out to the fleshy parts."8 Once the diseased part of the blood was separated, expulsion could occur. This "is performed all the rest of the time of the Disease, by means of these little Abscesses in the Flesh; for as they do not differ from the nature of abscesses, so they run through the same state of Crudity and Maturation, and dry up as others do; all which if they perform right, things go well, for the chiefest part of the Cure depends on these."9
Today, smallpox is understood to be contracted through the respiratory system after prolonged contact, first multiplying in the mucous system, then in the lymph system. So the idea that it was transmitted through the air was correct to a degree, although the air itself was not to blame. "Generally, direct and fairly prolonged face-to-face contact is required to spread smallpox from one person to another.
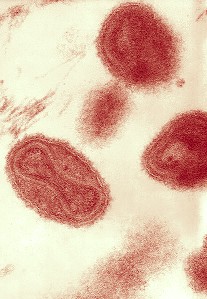
Image: CDC - Smallpox Virus Varions
Smallpox also can be spread through direct contact with infected bodily fluids or contaminated objects such as bedding or clothing. Rarely, smallpox has been spread by virus carried in the air in enclosed settings such as buildings, buses, and trains."10 Once in the respiratory system, the variola virus enters the bloodstream, gaining access to the internal organs while continuing to multiply. So Sydenham's notion that it was in the blood stream was also correct.
Aubrey and Harvey both took notice of the inability of smallpox to infect a person twice. Aubrey's explanation was simple: "Diseases that proceed from contagious Air, seldom or never affect the same Bodies twice."11 Since fevers were also thought to be transmitted by air by many physicians during this period, this seems like a strange conclusion for a doctor during this period to draw. Harvey's explanation was that people were 'seasoned' by the virus, something also associated with yellow fever. He ties it into his ideas about the pores of the humors being fit to receive the smallpox particles. "[T]he demipestiferous particles having formerly shaped the figures of the pores of those, that have thorowly been afflicted with the Small-pox, and finding free egress and regress, do not, or cannot fasten on their humors, or parts."12 Harvey was writing before it was determined that people could be intentionally infected with a case of smallpox through a early form of inoculation called 'variolation'; a process which was introduced in England and the American colonies during the golden age of piracy.
Both physicians Sydenham and Oliver suggested that there were different types of smallpox.

Artist: William Hoare
Physician William Oliver [with quill] (18th c.)
Sydenham begins by talking about two types of smallpox one of which he calls in 'distinct' and the other as 'confluent', 'flux' or 'fluxpox'. The descriptions referred to the appearance of the pocks - 'confluent' or 'flux pox' were pocks which merged with each other on the patient's body while distinct pocks did not. Sydenham suggests that "they differ not
essentially as they say, yet by some remarkable Symptoms which attend the one, and not the other, it is no hard matter to distinguish them."13 The primary difference between the two is that the action of the second type of smallpox is more violent than the distinct smallpox.
Oliver identifies three types of smallpox: the 'distinct', the 'middle sort' and the 'fluxt or confluent'. The first and last are basically the same as those identified by Sydenham. As their name suggests, the 'middle sort' sits between the other two types, having what Oliver explains are "all the Symptoms of the kind [distinct] sort, but in a greater degree, [and] the Pustules are small"14.
Today, four types of smallpox are recognized. The first is the ordinary smallpox, which was responsible for 85% of the smallpox cases. The second is the 'modified-type' smallpox which occurs on those who have been vaccinated. The symptoms can be the same, but once the pocks appear, the disease goes away more quickly. The third is the 'flat-type (malignant)' smallpox where the pox merge together and is accompanied by blood poisoning (toxemia). The fourth type is 'hemorrhagic smallpox' which has more severe symptoms leading to death, often before the pocks appear.15 From these descriptions, Oliver seems to have come the closest to identifying the types which are recognized today.
1 William Oliver, A Practical Essay on Fevers, 1704, p. 192; 2 Thomas Sydenham, The Whole Works, 3rd ed, 1701, p. 83; 3 Gideon Harvey, A Treatise of the Small pox and Measles, 1696, p. 29-30; 4 Thomas Aubrey, The sea-surgeon, 1729, p. 13; 5 Aubrey, p. 13-4; 6,7 Harvey, p. 30; 8 Sydenham, p. 87; 9 Sydenham, p. 87-8; 10 CDC, Smallpox Fact Sheet, 2004, p. 1; 11 Aubrey, p. 15; 12 Harvey, p. 32; 13 Sydenham, p. 78-9; 14 Oliver, p. 194; 15 CDC, "Smallpox: Clinical Disease", cdc.gov, gathered 2/27/19;
Conditions Conducive to Smallpox

Artist: Mary Beale
Physician Thomas Sydenham
(17th c.)
Although smallpox cases waxed and waned, it was always present in European society to some degree, which may explain why the doctors of this period didn't write as much about what conditions were needed to cause outbreaks of smallpox. English physician Thomas Sydenham noted that in 1661, smallpox "raged much about the beginning of May, but the Autumnal Epidemicks supervening, they retir’d."1 However, unlike some of the physicians describing similar viruses, he doesn't specifically pin smallpox to a certain time or season of the year, he merely mentions in passing that they started that year in May and tapered off as other diseases became more prevelant in the autumn. He also says that in 1667 and 1668, "the Small-Pox were more universal than I ever have I knew them before or since; and yet being gentle at that time, and of a good sort, they killed few, with respect to the great number of those that had them."2 Here, no season is mentioned, only that smallpox seemed to be widespread.
Modern physician and epidemiologist Donald R. Hopkins says that Sydenham espoused what he calls the 'miasmatic theory' of smallpox which suggests that the environment caused the disease. He explains that Sydenham "attributed the cause of smallpox to changes in the atmosphere, which assumed an 'epidemic constitution.'"3 This comes from the theory that air caused illnesses. Sydenham says that epidemic constitutions "proceed from a secret and inexplicable Alteration of the Air, infecting Mens Bodies... They continue as long as this secret Constitution of the Air, and no longer, neither do they come at any other time"4. So there was an environmental component to his ideas on how smallpox was transmitted..
Even the typically vocal physician Gideon Harvey has almost nothing to say about the conditions most suited to smallpox. He notes that there are two types, which he calls sporadic and epidemic. Harvey explains that the sporadic smallpox occur "when Persons at any time are scaterringly, that is, here and there surprised with either of these diseases [smallpox and measles]; which whereever they happen to seize many Persons in the same Country, about the same Seasons, and Times, become Epidemick"5. Note that he does not suggest that the epidemic form of smallpox occurs at a particular time or a particular place, just that when it occurs, it does so in epidemic fashion.
In fact, smallpox actually does have conditional aspects.
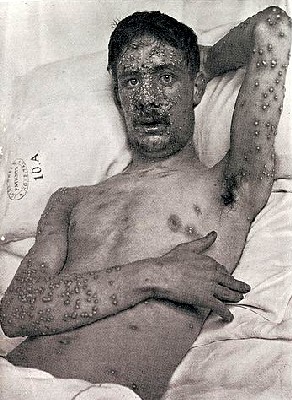
Patient with Smallpox, From "The Diagnosis of Smallpox",
Wellcome Collection (1908)
Hopkins says, "smallpox spread more rapidly during the winter months in temperate climates and during the dry season in tropical countries."6 This is precisely the sort of observation that many physicians from this time period typically made about epidemic illnesses, frequently incorrectly. Hopkins suggests that this seasonal aspect of smallpox "undoubtedly resulted from many factors, such as impaired mobility in tropical countries during the rainy season."7 However, he also points out that smallpox vaccacina virus has been shown by experiment to survive better in cool, dry conditions than in warm, wet ones, suggesting its affinity for certain climates.
The primary condition necessary for smallpox, however, is that it is contracted from other people who are infected. As modern doctor Michael Oldstone explains,
The individual with smallpox can transmit the infection at any time from a day before the rash appears until all the lesions have healed and the scabs have fallen off. During the early phase of the illness, the virus is transmitted from nasal secretions and cough. When the patient’s skin eruptions are fully formed, these lesions themselves also become a source of infectious material. Smallpox virus may contaminate clothing, bedding, dust, or other inanimate objects (fomites) and remain infectious for months.8
Curiously, this seems to have been understood by people to some degree before and during the golden age of piracy.

Artist: att to Gerard van Honthorst - Prince William II of Orange (1651)
As early as 1650, when Prince William of Orange II was diagnosed with smallpox, "his pregnant wife, who had not had smallpox, was not permitted to visit him. His mother was able to see her son during his illness since she had already had smallpox."9 In 1694, Queen Mary II of England contracted smallpox. Upon verifying this, she reportedly "gave orders that every lady of her bedchamber, every maid of honour, nay, every menial servant who had not had the smallpox should instantly leave Kensington House."10
This was even recognized by some men at sea. While in Myanmar, sailor Alexander Hamilton wrote that "the small Pox is dreaded or pestiferous, and in the Province of Kirian that Distemper is most dangerous and most infectious, so that if any one is seized by that Disease, all the Neighbourhood removes to two or three Miles Distance, and builds new Houses"11. He explains that this is not that difficult because their houses are made of bamboo and reeds. He further says that the villagers "leave with the diseased Person a Jar of Water, a Basket of raw Rice, and some earthen Pots to boyl it in, then they bid him farewell for twenty one Days."12 So they actually practiced a primitive form of quarantine. Another example comes from sailor Nathaniel Uring. After a couple of weeks shipboard with the virus while off the coast of Virginia, a local planter allowed him to rest in one of his out buildings. Even when he started feeling better, Uring explained, "I durst not go out of the Room, being charged [ordered] to the contrary, for fear I should meet some of the [planter's] Family and might infect them."13
From a physician's point-of-view, Hopkins says that "smallpox's contagiousness finally took hold after it was recognized by Jean Baptiste van Helmont (1578-1644) of Belgium, and Hermann Boerhaave (1668- 1738) of the Netherlands."14 While these men wrote well within the period of the golden age of piracy, new medical facts took a long time to get verified with physicians arguing strenuously about them, sometimes for decades.
1 Thomas Sydenham, The Whole Works, 3rd ed, 1701, p. 56; 2 Sydenham, p. 77; 3 Donald Hopkins, The Greatest Killer, 2002, p. 33; 4 Sydenham, p. 3; 5 Gideon Harvey, A Treatise of the Small pox and Measles, 1696, p. 28; 6 Hopkins, p. 8-9; 7 Hopkins, p. 5; 8 Michael B. A. Oldstone, Viruses, Plagues, and History, 2000, p. 35; 9 Hopkins, p. 35; 10 Thomas Babington Macaulay, The History of England, Volume IV, 1855, p. 530-1; 11 Alexander Hamilton, British sea-captain Alexander Hamilton's A new account of the East Indies, 17th-18th century, 2002, p. 356-6; 12 Hamilton, p. 366; 13 Nathaniel Uring, A history of the voyages and travels of Capt. Nathaniel Uring, 1928, p. 11; 14 Hopkins, p. 33
Smallpox Patient Symptoms
There are several descriptions of smallpox from this period. The physicians had quite a bit to say about the different types of smallpox they observed and the severity of the symptoms that occurred in each. English physician Thomas Sydenham discusses the symptoms of each of the two types of smallpox he identified in great detail, while fellow physician William Oliver gives only brief descriptions of his three types, two of which are the same as Sydenham's.

Early Smallpox Pustules, The Diagnosis of
Smallpox, Wellcome Collection (1908)
The first type discussed by both is the 'distinct' type, also referred to as the milder form of smallpox. Sydenham explains:
The distinct begin with shivering and coldness, which is presently followed by excessive heat [fever], a violent Pain in the Head and Back, Vomiting, a great propensity to sweat, (I mean in grown Persons)... a Pain at the Cavity of the Breast beneath the Region of the Heart, if it be pressed with the Hand, dullness and sleepiness, and sometimes convulsive Fits... The distinct Small-Pox usually come out on the fourth Day inclusively... at which time, for the most part, the Symptoms are very much abated or quite vanish, and the Patient thinks himself very well, only grown People are so disposed to sweat, that they can scarce be kept from it... which Disposition does not leave them, till the Pustles begin to ripen, and then it vanishes of its own accord. The eruption is after this manner; first Pimples as big as small Pin-heads here and there show themselves, and first of in the Face, or Neck and Breast, and afterwards in the whole Body. At this time the Jaws are affected with a pain that increases as the Pustles rise, which growing daily bigger and higher inflame the neighbouring Skin and Flesh.1
Sydenham here gives a very detailed and wandering description of the pocks, basically noting that the area between them goes from white to red accompanied by sharp pain, they then swell, first on the face, then on the hands, eventually coming to a head and ejecting the white/yellow pus contained in them. "On the eleventh day, the Tumor and Inflammation of the Face manifestly diminish, and the Pustles of the Face and Body... dry away and fall off: And in this sort of Small-Pox, most commonly vanish on the fourteenth or fifteenth day... Scurfie [dry and loose] Scales succeed the Pustles of the Face, and sometimes Pock-holes follow them"2. He says that the pocks are about the size of a dried pea and that the patient is usually constipated while ill.
Oliver doesn't provide near as much detail, getting right to the point. He explains that "the Pustules are large, few, and separated at a distance
Patient and Physician, From Elementarwerke fur
die
Jugend und ihre Freunde (1774)
from one another; appear the Fourth Day, and are at their Height the Eighth." His list of symptoms include "some Uneasiness, Pains of the Head and Back, Fever, Sickness at Stomach, and sometimes a little vomiting". The pocks (or pustules) form pus on the eight day, "when the second Fever comes on, and then the Face and Hands swell, and all goes off in a few days."3
Sydenham discusses his second type of smallpox - the confluent or flux-pox - in similar, extensive detail. He begins by explaining the symptoms are essentially the same as those of the distinct pox, "only they are more violent, the Sickness, Vomiting, Fever, and the Restlessness, rage more cruelly... only the Sick is not so apt to sweat in this sort"4. He notes that patients in this type of smallpox have diarrhea rather than constipation. He says adult patients also salivate a great deal, which begin either with appearance of the pocks or a day or two after. "First the Matter is thin, and easily spit up... but commonly about the eleventh Day it is more clammy, so that it is difficulty hawked up; the Sick is thirsty, and now and then Coughs as he drinks, and the Liquor flies out at his Nostrils; and after the Day Salivation most commonly ceases"5.
The pocks usually appeared within three days, although they could take as many five. They are accompanied by pain in the loins,

Photo: CDC
Flat Type Smallpox, With 'Bladder-Like' Pocks
Similar
to Sydenham's
Description
stomach or limbs. Unlike the distinct smallpox, Sydenham says that the fever continues for many days following the appearance of the pocks. About the appearance of the pocks in the fluxpox, he explains
these do not rise so high as the distinct [smallpox do], especially those in the Face; but being entangled one with another, first they represent a red Bladder that covers the whole Face, which they sooner tumifie [swell] than the distinct are wont to do, and afterwards they are like a white Skin glu’d as it were to the Face, which does not rise much higher than the common Superficies [surface] of the Skin. After the eighth Day, the white Skin increases daily, till at length it falls off in large Scales.6
Sydenham warns that the scales "are indeed very corrosive; for they do not only pit, as the distinct Small-Pox used to do, but imprint also filthiy Scars on the Face; and if the Flux-Pox have been very violent, the Skin of the Shoulders and Back is also sometimes marked"7.
As before, Oliver is concise in his description of the fluxpox, which generally agrees with the one given by Sydenham. "These run over all the Face, in one Cluster, and nothing can be put between them; are often hard and horny, and always very dangerous: The Symptoms are all the same with the former, but severer... They Salivate very much, and recover with a great deal of difficulty. The Critical Day in this sort of

Aztec with Small Pox, Florentine Codex (16th century)
Small-Pox is the 11th, sometimes the 14th, 17th, 21st."8 He also mentions that the pocks in fluxpox take longer to open and dry up.
Since Oliver is the only physician to discuss the 'middle sort', his is the only description of that type. He explains that the pocks are less defined than the distinct pox and some of them touch like those seen in the fluxpox, appearing on the third day and continuing to be active about the eleventh. The other symptoms are a mixture of the two as well. They are "attended with a brisk Fever, and all the Symptoms of the kind sort, but in a greater degree, the Pustules are small, and they are seldom without a Salivation, which towards the end, when the Spittle grows thick, is very troublesome, and many are quite choak'd with the thick Phlegm that lies in their Throats."9
Smallpox is included in one of sea surgeon John Moyle's books, although he doesn't distinguish between types. His symptoms generally agree with

Sea Surgeon John Moyle (1683)
some of those discussed by the physicians in the distinct pox. Moyle says smallpox patients
are usually taken at first with a dulness or heaviness, and then a pain in the back, with grievous Head-ach. ...No matter although he doth not go to Stool in four or five dayes; give him no Clyster [enema] for all that, least you should make him take cold: For about the first crisis he will go to Stool of himself, which is about the seventh day from his falling sick. ...[the pocks] will come out by the third day.... If through some ill accident, or the great malignity of the Distemper he hath not miscarried before, he will have them [the pocks] at the height before the fourteenth day, and then recover: But in his recovering, let him have a care of falling into a relapse by heedlesness... let him not scratch off the scurf [left by the pocks] with his hands, for by these things the Scarrs will be deep10
Moyle was an eminently practical doctor whose descriptions are simple and straightforward. He focuses primarily on the cure. This involved clysters, bleeding and possibly purging once smallpox was confirmed, good food and drink such as strong beer and sack [fortified wine] and giving the patient as much fresh air as possible. (With the exception of strong beer and sack, these recommendations are also given by Sydenham.) Moyle suggested using very few medicines, rather letting the disease work its way through the patient naturally. Interestingly, smallpox only appears in his first book, Abstractum Chirurgæ Marinæ, printed in 1686. His second book, which went through two printings in 1693 and 1703, does not include a description of this virus.
Merchant sailor Nathaniel Uring came down with small pox while anchored near the Rappahannock River in Virginia in 1699. He says that he was 'extremely sick' and 'delirious' for several days.
Artist: Gustav Dore
"I fell down aswound", From Rime of the Ancient Mariner (1876)
They had no surgeon aboard, so the captain gave him saffron infused in warm rum punch, "by which I found great Benefit; for soon after I drank it I had a Stomach to eat"11. He started to feel better (something mentioned by Sydenham), "and the Small-Pox came out very kindly, nor had I any Sickness at my heart any more."12 He mentions being very cold, most likely a symptom of fever. A woman on land "was so good as to send me some Rum, a little Saffron, and a Couple of Fowls for my Refreshment, but would by no Means allow me to go to her House for fear of infecting her Family."13 He was eventually placed in a small out building on land, being "so very weak, that I could hardly stand... [experiencing] great Trouble and Pain" in the journey. Once there, he quickly revived, it being warm and dry as opposed to the cold and wet conditions on his ship.
Today, the CDC says that smallpox begins with an incubation period during which the afflicted have no symptoms, lasting anywhere from 7-19 days. Of course, this would not have been noticed during the golden age of piracy. The first symptoms that appear are a high fever, head and body aches and vomiting, which last two to four days. This stage may also include weakness, abdominal pain, chills and anorexia.14 The first rash appears in the mouth and on the tongue, starting as spots which break open. The rash spreads to the face and then to the rest of the body within twenty-four hours, after which the patient begins to feel better. About four days after the mouth rash appears, the pocks on the body fill with fluid and the fever may return. In five to six days, the pocks then become pustules, "sharply raised, usually round and firm to the touch, like peas under the skin", form a crust and then scab by about the tenth day. These scabs fall off, with most of them being gone within about three to four weeks from the initial appearance of the first rash. The patient is contagious throughout those weeks.15 With the exception of the diarrhea and salivating, these symptoms agree with those mentioned by the period doctors.

Photo: CDC - Hemorrhagic Smallpox
The other three types of smallpox mentioned by the CDC include the modified-type, flat-type (malignant) and hemorrhagic. The modified type has all the same symptoms as above until the rash appears. In this case, the pocks only take about ten days to fill and scab and patients are less likely to have fever once the rash starts. In the flat type (malignant) smallpox, "the skin lesions in this type develop slowly, merge together, and remain flat and soft (often described as “velvety” to the touch). They never progress to the pustular stage." This sounds in many ways like the fluxpox described by Sydenham and Oliver. Hemorrhagic small pox symptoms appear more quickly with more severe fever, headaches and abdominal pain. The skin turns red and may hemorrhage. "Death usually occurs by the 5th or 6th day of the rash, often before characteristic smallpox lesions develop. Death results from a profound toxemia, leading to multi-organ failure."16 This again has elements of the fluxpox, possibly because period physicians were unable to differentiate between the two types.
1 Thomas Sydenham, The Whole Works, 3rd ed, 1701, p. 79-80; 2 Sydenham, p. 80; 3 William Oliver, A Practical Essay on Fevers, 1704, p. 192; 4 Sydenham, p. 81; 5,6,7 Sydenham, p. 83; 8 Oliver,p. 195; 9 Oliver,p. 194-5; 10 John Moyle, Abstractum Chirurgæ Marinæ, 1686, p. 123-6; 11,12 Nathaniel Uring, A history of the voyages and travels of Capt. Nathaniel Uring, 1928, p. 9; 13 Uring, p. 9-10; 14 CDC, "Smallpox: Clinical Disease", cdc.gov, gathered 2/28/19; 15 CDC, "Smallpox: Signs and Symptoms", cdc.gov, gathered 2/28/19; 16 CDC, "Smallpox: Clinical Disease", cdc.gov, gathered 2/28/19
Smallpox Patient Signs of Impending Mortality
Among Thomas Sydenham's comments are that the smallpox was not generally to be considered life-threatening unless there were a lot of pocks on the face of a patient with fluxpox. In such a case, "the Sick is in as much danger as if every Member was crouded with them; and on the contrary, tho’ the Trunk and Members be very full,

Artist: Gustav Dore
Ill Men on Ship's Deck, From Rime of the Ancient Mariner (1876)
if there be but few of them in the face, there is less danger."1 He explains that patients with fluxpox typically stop salivating on the eleventh day after the appearance of the pox and, "unless the swelling in the Face persists a little longer, and that of the Hands, now manifestly beginning, supplies [takes] its Place, the Sick must necessarily die"2. He also warns that as salivation progresses, it can go from being 'crude and thin' to 'viscid and tough' "so that the sick is in danger of being choaked, and his Drink is like to strangle him, so that it is forced back through his Nostrils with a violent Cough; he is hoarse, and seized with a great dullness, being wholly oppressed by the violence of this Disease, and most commonly dies in such an Agony"3.
Sydenham also warns that patients with the distinct smallpox are in danger when 'irregular symptoms' occur on the eighth day after the pocks first appear, such as failing to sweat at that time because the 'venom of the disease' is not being ejected from the body. If the patient's face "appears flaccid and white, yet the Pustles continue red and elevated... and the Sweat, which followed freely to this Day, now ceases of a sudden, with Anxiety, violent Sickness and Restlessness, he makes Water often, but a little at a time" then the patient will soon die.4
William Oliver warns that spots in between the pustules which "incline to a Purple. Bloudy Urine, or any Hæmorrhage

Photo: CDC - Severe Hemorrhagic Smallpox
whatsoever" are 'very bad'.5 He also says that when the smallpox occurs, "any uncommon Pains disguise the Distemper, [and] that the Patient is severely seiz' d, and seldom escapes, and if he does 'tis with all the difficulty in the World"6.
Modern texts suggest some of the signs of impending mortality in smallpox. Physician and researcher Donald Hopkins explains that when smallpox onset is sudden and severe
death usually occurred within three to five days, often caused by overwhelming toxemia or massive hemorrhaging into the skin, throat, lung, intestine, or uterus. Such patients had no characteristic papular or vesicular eruption, only a nonspecific red or violet patchy, petechial [red or purple spots], or morbilliform [measle-like] rash such as may be seen in many other severe infections where natural clotting mechanisms are thrown into chaos. In other malignant infections, the smallpox virus caused diffuse destruction in the dermis, or deeper layer of the skin, and patients died between ten and fourteen days after onset of symptoms, with pustular lesions that were sometimes confluent [merging with each other].7
These first symptoms described by Hopkins correspond with the flat type, while the second symptoms are indicative of the hemorrhagic smallpox. They also agree fairly well with the symptoms described by Sydenham and Oliver.
1 Thomas Sydenham, The Whole Works, 3rd ed, 1701, p. 82-3; 2,3 Sydenham, p. 85; 4 Sydenham, p. 84; 5 William Oliver, A Practical Essay on Fevers, 1704, p. 197; 6 Oliver, p. 198; 7 Donald Hopkins, The Greatest Killer, 2002, p. 5
New World Quarantine Page Menu: 1 2 3 4 5 6 7 8 9 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-