

Simple Wound Care Page Menu: 1 2 3 4 5 6 Next>>
Simple Wound Care in the Golden Age of Piracy, Page 3
Simple Broken Skin Wound Care

Instructing Surgical Students, From Cours d'Operations, Pierre Dionis (1708)
As explained, there were five theoretical steps in caring for simple broken skin wounds during the golden age of piracy, as first proposed by Guy de Chauliac.
Succinctly stated, they are:
Step 1: Remove foreign objects.
Step 2: Bring the wound lips together.
Step
3: Keep the wound lips together.
Step 4:
Maintain wound temperament.
Step 5:
Remedy complications.
This sounds very clean and neat, but the healing process for wounds described by surgeons during this period contains a variety of other necessary steps that are not directly addressed in this model. However, many of the other aspects of the healing process for simple unbroken skin wounds were either specifically included in or implied as being a part of these 5 steps.
Step 1 of Simple Broken Skin Wound Care: Remove Foreign Objects
This step appears to be quite straightforward, although the word 'foreign' may not be strictly accurate. As French surgeon Ambroise Paré explained, things to be removed from a wound may "have come from without, or from within the body"1.

Photo: Author's Collection
Forceps For Foreign Object Extraction
Military surgeon Richard Wiseman's laundry list of items to be removed proves this; he includes "concrete[d] Bloud, Hair, Sand, Dust, pieces of Bones, Cartilages, or pieces of the Weapons, Rags, &c. [etc.]"2 However, several other things are recommended when treating cuts and other divided skin wounds by surgical authors which fit neatly into this category.
The first sub step of removing foreign objects is to cleanse wounds. Although this is not suggested as a regular step in the wound cure process, Wiseman and sea surgeon John Moyle both mention it when describing treatment during some of their case studies. Wiseman notes that when he encounters "Wounds that are full of Maggots or Worms [they] ought to be washt with a Decoction , card. benedict. [blessed thistle] rad. gentian. [gentian root] Myrrh, aloes, &c. and deterged [thoroughly cleansed] ...with Mundificatives [cleansing medicines]: after which you may proceed in the same method of Cure"3. Other cleansing agents are suggested by sea surgeon John Moyle in one of his case studies, where he advises the surgeon to "wash it [the wound] well with Wine, or Spirit of Wine"4.
The second sub step of removing objects from a wound is mentioned by Wiseman - increasing the size of a wound when treating deep cuts. As he explains, "If the Wound be deep, and the Orifice narrow, yet capable of inlarging; it must be laid open proportionably, that the Matter may not be retained, and render the Wound more hollow."5
He recommends opening the wound by first trying a caustic - a stone or medicine that can burn the wound open. If that doesn't work, Wiseman suggests using a knife or scalpel. If neither of those methods manage to completely open the wound, he suggests using "a Seton-needle with a twisted Silk or Thread" to create a fontanel.6 The seton needle would be used to feed the silk or thread through the two lips of the wound, often after placing a pea inside the wound to keep it open. The thread and pea would irritate the wound, causing it to become infected and release matter, "till Nature shall be disposed by the Physician's help to heal the internal Viscera [organs], and then the external Ulcer will heal of it self under the Pea if you leave it not timely out."7
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 253; 2 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 340; 3 Wiseman, p. 349; 4 John Moyle, Abstractum Chirurgæ Marinæ, 1686, p. 60; 5,6 Wiseman, p. 350; 7 Wiseman, p. 203
Step 2 of Simple Broken Skin Wound Care: Bring the Wound Lips Together
This second step is a curious addition to the process given that it could be easily combined with Step 3 ('Keep the wound lips together.') without losing any information.
Artist: David Ryckaert
At The Village Barber Surgeons (17thc)
Richard Wiseman says that this step "is delivered in a few words, but they are to be observed as a Law; for without that Reduction [restoration] in the Lips, a flow and deformed Healing follows."1 His recognition that there is little more to say almost sounds as if he also questions de Chauliac's decision to make this an individual step. Even revered French surgeon Ambroise Paré admits that "the Surgeon shall attaine to the second and third scope [steps] of curing wounds by two and the same meanes, that is, by ligatures [binding the wound tightly] and suture"2.
Still, Wiseman recommends that the wound edges "are to be brought together gently and equally, that they may touch one another, and so be prepared for Unition."3 And Paré says that if the edges of the wound aren't evenly matched, they won't reunite.4 German surgeon Matthias Gottfried Purmann advises the surgeon to "draw the Lips of the Wound as near together as possible, and then dress it artificially, that the circulating Liquors [indirectly referring to humors] may not go out at the lacerate[d] and wounded Ramuli [nerves or blood vessels], and so prevent its Healing."5
Wiseman also adds that when a "Wound hath lain long undressed... and be now so contracted and stubborn that the Lips of it will not be brought near one another; you must then foment them warm with some lenient [softening] Decoction"6. He recommends one made from the leaves and roots of marshmallow and violets, flax seeds, combined with fresh milk.
1 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 341; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254; 3 Wiseman, p. 342; 4 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254; 5 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 181; 6 Wiseman, p. 349
Step 3 of Simple Broken Skin Wound Care: Keep the Wound Lips Together
Keeping the lips of the wound together is a multifaceted step, containing three parts. The first part involves preparing the wound for healing. The second part involves securing the lips of the wound so that they remain together. The last part involves encouraging the regeneration of flesh in the secured wound. Let's look at these in detail.
Preparing the Wound Site for Closure
This first part of holding the two sides of the divided skin together is concerned with preparing the wound site for healing. There are a couple of different subparts to consider. The first shouldn't surprise anyone who has taken a first aid class: the bleeding in a wound must be stopped. Paré explains that before the lips of a wound can be secured, the surgeon "must well observe whether there be any great fluxe of blood present, for he shall stoppe it if it be too violent"1.
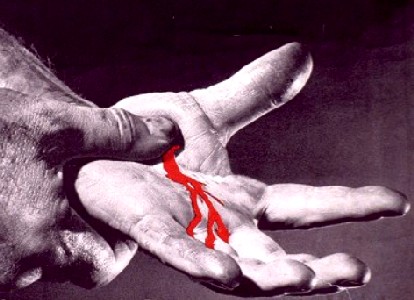
Photo: Liberty Mutual Insurance - Stopping Bleeding
Richard Wiseman suggests that bleeding in a wound is stopped "by bringing the Lips of the Wound close together by Suture" and by the application of 'drying and agglutinating' medicines as well as covering the wound with a compress and bandage. His suggested medicinal is composed of powdered aloes and frankincense which is then combined with rabbit's fur and egg white.2
To curb blood loss in a wound, sea surgeon James Yonge recommends the use of turpentine, explaining that it is good "especially [for] restraining the fluxes of bloud, without the pain, burning, Synovia [release of fluid], prolixity [excess], flux [flow] of matter, and all or most the other ill accidents"3. Yonge then details the use of turpentine in the case of a sailor who accidentally "thrust the point of a Knife deep into his hand... [T]he bloud spouted out very impetuously; heating some Ol. Terebinthinæ in my Uvula spoon [a small spoon for holding down the uvula], I poured it into the bleeding Wound, which immediately stopped it"4.
Of course, such methods were employed only when the surgeon actually wanted to stop the bleeding in a wound. Unlike today's first aid procedure, several surgical authors advised that a wound should not only be allowed but encouraged to bleed at times.
When treating a broken skin wound, Paré advises the surgeon to "provoke it, if [it bleed] too slow, (unlesse by chance it shall be powred out into any capacity or belly) that so the part freed from the superfluous quantity of blood may be lesse subject to inflammation"5. In a related comment, John Moyle recommends that washing a wound be performed only after it "has done bleeding"6. Richard Wiseman has the most to say about allowing bleeding in a new wound, recommending that the surgeon "permit the Wound to bleed, accordingly as you in your judgment shall think fit, still having respect to the Constitution and Habit of body, that what is in the small Veins cut a sunder may flow out, as well to hinder Inflammation, as the generation of much Matter."7

Photo: Wiki User Sumasla - Allowing a Wound to Bleed
Although not directly stated in these recommendations, the purpose of letting a wound bleed itself out concerns one of the bodily humors: blood. Humor theory suggests that blood can become corrupted at a wound site. Allowing the wound to bleed served the same purpose as intentionally letting blood - it prevented the corruption of blood humors which, if left to corrupt would eventually produce inflammation. Wiseman's additional suggestion that bleeding prevented 'generation of much Matter' also highlights the concern with 'bad' humors. Descriptions of corrupted at a wound site included 'gleet' (discharge from a wound) and pus - both generated matter. Even Wiseman's comment on deferring bleeding in a wound according to the 'Constitution and Habit of body' is related to humors. Different body types were considered to have an excess of some humors and a lack of others and these things were taken into account when deciding how much blood a person could feasibly be allowed to lose in the effort to purge the unwanted corrupt humors.
Wiseman has a few other suggestions for preparing an open wound site for closure. "The Bleeding staid, if there be Hair growing about the Wound, shave it off: then wipe away the clotted Bloud with a Sponge dipt in Red wine, Oxycrate [water and vinegar], or Water."8 Here again we find a recommendation for cleaning the wound. Wiseman also warns the reader to be careful in removing the clotted blood for deep inside the wound, "for thereby you may stir up a new Bleeding; whereas this concreted Bloud keeps the Wound warm, and defends it from the outward Air; and by digestion Nature will thrust it forth."9 'Bad' air was believed to cause health problems; exposure of wounds to air was thought to accelerate corruption in them.
Once these preparatory steps had been taken the wound lips could be secured.
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254; 2 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 351-2; 3 James Yonge, Currus Triumpalis, é Terebinthô., p. 65; 4 Yonge, p. 78; 5 Paré, p. 254; 6 John Moyle, Abstractum Chirurgæ Marinæ, 1686, p. 60; 7,8,9 Wiseman,p. 341
Securing the Wound Lips
The edges of an open wound had to be secured by the surgeon to allow their healing to begin, as the action in this step indicates. Three different methods were discussed by surgical authors from this period for maintaining the wound edge contact: suturing (both regular and dry suturing), glue and bandaging.
Securing the Wound Lips - Regular Suturing
Suturing had an important place in keeping the lips of the wound together during the golden age of piracy. Late 16th century English military surgeon William Clowes said that "all good authors command to stitch wounds of necessity, otherwise it would cause a great deformity."1

Artist: Thomas Eakins
Suturing a Wound, The Gross Clinic (1875)
Sea surgeon John Moyle explains the elements of suturing a wound, beginning with the wound lips being brought together
as even as possible, and that the extremities of the Vessels may meet even also; and stitch the Wound with a fine Needle and Silk, passed through Diapalma Plaster [a plaster of palm-oil, litharge, and sulphate of zinc] (which is better than Wax) have a care in your stitching that you take only the Skin, and do not puncture the Nerves or Tendons, nor Muscles, for that would cause ill accidents.
And let your stitches be something wider at the depending part of the Wound, that there may be way for the Blood and Matter to come forth.2
You will notice that concern about material forming in the wound in Moyle's description.
William Clowes also describes the process, noting that the suture should be performed with "a sharp and square pointed needle, with a strong , even and smooth silk thread, well waxed." He starts the suture in the middle of the wound, using only a few stitches, not too close together because he doesn't "think it good to make the stitches too thick, because they do oftentimes stir up accidents, as pain and inflammation". Like Moyle, he leaves "a decent place for the wound to purge at"3.
Richard Wiseman talks about the type of stitch used, recommending the surgeon "endeavour the bringing of the Lips together by the Incarnative Suture, making so many Stitches as may retain them together". He adds that "if you doubt this way not sufficient, you may...
_Olek_Remesz.jpg)
Artist: Olek Remesz
Incarnative Suture (Simple Interrupted)
pass Needles or Pins through the Lips of the Wound, with little Plates of Lead to secure them from tearing [the surrounding skin]."4
You will note that Wiseman specifies an incarnative stitch. The terminology of suture types varied somewhat depending on who was explaining the process. This can make understanding the type of stitch each author recommends a bit challenging. In addition, different authors suggest different suturing material as well as variations in the way a suture should be made and/or tied. For those interested in an in depth discussion of sutures and their terminology, see this page. For those not so inclined, see the image shown at left for a general idea of what Wiseman is talking about.
French surgeon Ambroise Paré is a little less enthusiastic in recommending suturing of simple wounds, suggesting that the use of bandaging (which he refers to as 'ligature') to keep the wound lips together is sometimes preferable. He does say that a wound "which divides the Muscles tranversly [across], stands in need of both Suture and Ligature; that so the lips which are somewhat far distant from each other, and as it were drawn towards their beginning, and ends may be conjoyned."5
Paré also states that when treating wounds where
any portion of a fleshy substance by reason of some great cut shall hang downe, it must necessarily be adjoyned and kept in the place by suture. The more notable and large Wounds of all the parts, stand in need of Suture, which doe not easily admit a Ligature [bandage], by reason of the figure and site of the part which they are as the Eares, Nose, Hairy-scalpe, Eie-liddes, Lippes, Belly and Throat.6
1 William Clowes, Selected Writings of William Clowes, p. 111; 2 John Moyle, The Sea Chirurgeon, 1693, p. 66; 3 Clowes, p. 107-8; 4 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 349; 5,6 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254
Securing the Wound Lips - Dry Suturing and Wounds of the Face
Dry suturing was a special type of stitch which "is used alone in the Face, as making the least Scar."1 The key to dry stitching was to attach an adhesive plaster to the undamaged skin on either side of the incised wound with the edge of the plaster closest to the wound not being adhered to the skin. Sea surgeon John Atkins advised the surgeon to use "a very sticking Gum or Plaister, spread on Leather close to the Lips of the Wound"2. One the adhesives dried, the the two
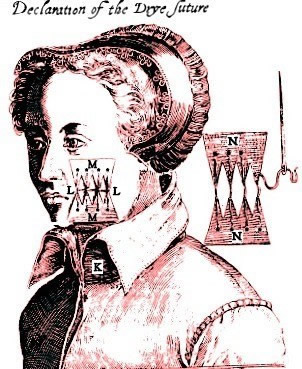
Guillemeau's Dry Suture Diagram, From Jacques
Guillemeau's The French Chirurgerie (1597)
'free' edges of the plaster were sewed together, drawing the wound lips close without actually puncturing them.3
While Atkins discusses the dry suture in his book, fellow sea surgeon John Woodall advises against its use stating, "I will not stand to teach the drie stitch here, for it is not proper at sea, it fits the land better."4 He does not expand on his reasons for this, however. While sea surgeon John Moyle uses a plaster in his comments on wounds of the face and head, he still pierces the skin, warning the surgeon to take "care that you stitch the Skin only, and not puncture the Muscle"5. In fact, his comments on suturing wounds of the face mirror those of other wounds cited in the previous section. In his previous book, Moyle seems more interested in the needle, noting in his previous book that it should "be fine and slender, that there may not be an ugly scar afterward."6
Part of this casual attitude towards sutures of the face may have something to do with the patients. Sailors were sturdy customers who probably weren't as concerned about disfiguring as others. In fact, Richard Wiseman goes to great pains to minimize the use of regular suturing and instead rely on a dry suture for a lady who "was wounded down the whole length of the Forehead to the Nose also transverse the left Eye-brow to the Temporal Muscle"7. However, in the case of the sailor who had had a cross carved into his face for 'prating on' about religion as described on the first page of this article, Wiseman didn't bother with the dry suture, simply stitching the wound. As he explains, "The Patient was well pleased with his Cure, though there remained some marks of a Cross. These sort of people wearing them with much pride in their Faces, as marks of their Courage."8
1,2 John Atkins, The Navy Surgeon, 1742, p. 64; 2 John Kirkup, The Evolution of Surgical Instruments; An Illustrated History from Ancient Time to the Twentieth Century, 2005, p. 335; 4 John Woodall, the surgions mate, 1617, p. 137; 5 John Moyle, The Sea Chirurgeon, 1693, p. 77; 6 John Moyle, Abstractum Chirurgæ Marinæ, 1686, p. 24; 7 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 361; 8 Wiseman, p. 362
Securing the Wound Lips - Gluing

Matthias Gottfried Purmann
German surgeon Matthias Gottfried Purmann suggests an interesting alternative to stitching a wound which he learned from a quack surgeon - using glue to stick the edges of the wound together. He mentions two types of glue in his book for joining skin - joiner's glue - used by craftsmen to glue things such as wood, leather and other materials together - and plant-based glues.
Although this method would have been a quick and convenient way to fix minor wounds on a ship, it was not likely to have had widespread use during this time. Purmann is the only author under study to discuss it. Even he is somewhat circumspect in his praise. While he ends his commentary on the practice with "whoseoever practices [this method of gluing wounds), will find such Benefit by it, that he will never change it"1, he doesn't actually admit to the reader that he even tried the method.
For a more complete look at Purmann's discussion on gluing wounds, see this page.
1 Matthias Gottfried Purmann, Churgia Curiosa, 1706, p. 181
Securing the Wound Lips - Bandaging
The third method for securing the edges of a wound together was by bandaging. Military surgeon Richard Wiseman only recommends bandaging where "the Wound be small, and in a Fleshy part, & according to the length" of the wound site. He goes on to say that bandages work in such cases because "Nature will truly act her part, by application of bloud and nourishment to both sides indifferently and finish the Coalitus [reunion of the parts] without your farther assistence."1

Feeling by Adriaen Brouwer (1635)
Ambroise Paré agrees, explaining, "For a simple and small solution of continuity [divided skin wound], stands only in need of the Ligature which we cal incarnative, especially, if it be in the Arms or Legs"2. Sea surgeon John Atkins adds his approval, explaining that "Wounds superficial or short, need no stitching"3.
Sea surgeon John Moyle uses bandaging in his explanation for how to heal a 'great Wound in a Musculous Part, with loss of substance'. When the wound is deep, it becomes necessary to allow the wound to 'incarn' or generate flesh from the bottom of the wound upwards. Stitches would be inappropriate because the wound would heal at the top before the deeper parts of the wounds could fill with new flesh, leaving an abscess. Moyle notes that he places 'Buttons' (small pieces of lint formed like a button) soaked in medicines which stop the bleeding and encourage the formation of new flesh in such wounds. These were to be removed in two days, something that couldn't easily be done if the wound was sutured.4
Fellow sea surgeon John Atkins agrees with Moyle, stating "I never stitched any of these large incised Wounds... but I [later] found myself obliged in two or three Days, by the Tumor and Inflammation [caused], to cut them [the stitches] out again". He goes on to say that even if the "Stitches could be kept in longer, that will not prevent the Wound's gaping in the same manner, when they at last do come out."5
Paré advises the use of sutures in deep wound, but with a twist to solve the problem identified by Moyle and Atkins. He tells the surgeon "you must take up much flesh with your needle; for if you only take hold of the upper part, the Wound is only superficially healed:but the matter [will be] shut up,and gathered together in the bottome of the Wound, [which] will cause abscesses and hollow Ulcers"6.

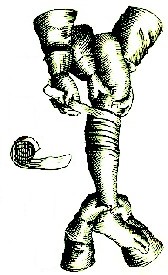
Bandaged Leg, From Opus Chyrurgicum Artzney Buch, p. 10 (1565)
The general policy seems to use bandaging over stitches when dealing with divided skin wounds except for minor wounds and possibly deep wounds where anything is physically inserted into the wound.
This brings up another point which most of the authors who discuss it agree upon: tents (folded pieces of lint) should not be packed into wounds. Wiseman speaks against it, warning that surgeons "must not lay a Pledgit, or croud a Dossil of Lint or Tent into a little Wound; no, that is the way to keep the Wound open, and make it painful, whereby Defluxions [discharges] are stirred up, the Temperament of the Part weakened, and the Cure prolonged; contrary to the intention of all who have writ of Wounds, and to the practice of our knowing Chirurgeons here."7
Even John Moyle, who advised using small buttons of lint in deep wounds, comes out against this, saying "let me forewarn you here that you do not cram up such a Wound as this, with restringent Dorcels [dossils], or any other Medicines, to the bottom, and within it; for then the Vessels would never unite, nor would the Wound be kindly healed"8.
1 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 342; 2 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254; 3 John Atkins, The Navy Surgeon, 1742, p. 164; 4 John Moyle, The Sea Chirurgeon, 1693, p. 62-3; 5 Atkins, p. 164; 6 Paré, p. 255; 7 Wiseman, p. 342; 8 Moyle, p. 68
Securing the Wound Lips - Wound Bandage Types
Richard Wiseman and Ambroise Paré discuss three types of bandages used on wounds at this time. Wiseman explains that these were recommended "by the joynt consent of all the Ancients [ancient surgeons and physicians]."1 The three types of bandages were: incarnative, expulsive and retentive ligatures.
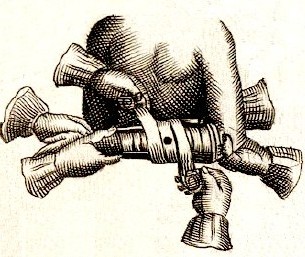
The Incarnative Ligature, From The Chyrurgeons
Storehouse,
by Johannes Scultetus, p. 68 (1653)
The incarnative ligature (also called by Paré the glutinative ligature) was used on simple wounds that were still bleeding. It is made by taking a roller bandage and rolling each end until they met in the middle. The middle of the bandage was then placed "on the part which is opposite to the Wound, to prevent pain and inflammation" which could have been caused if the middle of the bandage was placed directly upon the wound.2 The two rolled sides of the bandage were then to be unrolled around the part, going "upwards, partly crossing it, and going downewards againe, [so that] we may closely joyne together the lippes of the Wound."3 (See the image at left.) Both authors warn not to make this bandage too tight (for fear of hurting the patient and inflaming the wound), nor too loose (for fear of it not holding the wound lips together).
The Expulsive Ligature,
From
The Chyrurgeons
Storehouse,
by Johannes
Scultetus, p. 106 (1653)
The explusive ligature was used to push unwanted bodily humors and their generated matter out of a wound as well as to prevent new humors from being able to get to the wound. It was made using a roller bandage, the end of which is put "beneath the seat of the Humours [at a point below the wound farthest from the trunk of the body], and rowl it upwards pretty streight [tight] at first, and by degrees; as you come nearer the Mouth of the Wound, gentler and gentler."4 The purpose in easing up on the bandage as you got near the wound was so that "the sanious matter [serum, pus and other such humors] may be pressed forth."5 After the roller passes over the wound, the surgeon must roll "harder, and yet a little streighter [tighter], the higher you go, to hinder the descent of Humours; but not too hard, for fear of harm."6
The retentive ligature is used on "such parts as cannot suffer straight [tight] binding, such are the Throat, Belly, as also all parts oppressed with paine... The use thereof, is to hold to locall Medicines [topical medicine]."7 Little is said by either author about the method for making such a bandage. Given their purpose, they would have most closely resemble modern cloth bandages.
Both authors finish by discussing the type of material that should be used for the bandage/ligature. Wiseman says, "they must: be made of good strong even Cloath, white, clean, and gentle, without Hem, Seam, or thread hanging by."8 Paré adds that roller bandages "ought to be of linnen and such as is neither too new, nor too old; neither too coarse, nor too fine."9
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 254; 2 Richard Wiseman, Severall Chirurgicall Treatises, 1676, p. 343;3 Paré, p. 254; 4 Wiseman, p. 343; 5 Paré, p. 254; 6 Wiseman, p. 343; 7 Paré, p. 254; 8 Wiseman, p. 344; 9 Paré, p. 254
Simple Wound Care Page Menu: 1 2 3 4 5 6 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-