

Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Treating Sprains & Dislocations in the Golden Age of Piracy, Page 11
Specific Dislocation/Luxation Cure: Knee
"Owing to their configuration, the bones at the knee are indeed frequently dislocated, but they are easily reduced, for not great inflammation follows, nor any constriction of the joint." (Hippocrates, The Genuine Works of Hippocrates, Volume 2, 1849, p. 546)
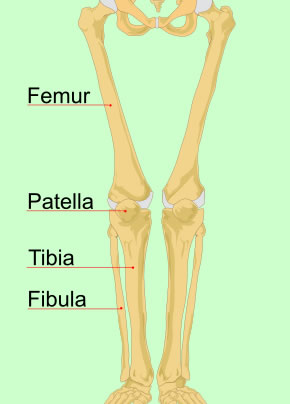
Image: Mariana Ruiz Villarreal - Leg Bones
Sea surgeons John Atkins and James Handley, English surgeon Richard Wiseman and French surgeon Ambroise Paré all discuss methods for repairing dislocations of the knee. Sea surgeon John Woodall mentions it when explaining the use of his commander, but doesn't provide any detail on the process.1
All of the other authors agree that the knee can be luxated or sub-luxated to either side and backwards, but it "doth scarce admit of any Luxation forward, unless the cause be exceeding violent."2 Atkins says this is because of the position of the patella (knee cap) and the fact that it is difficult to bend forward far enough to displace. Paré explains that "the cavitie of the leg-bone [tibia] is superficiarie [superficial] and very smooth, but the cavitie of the lower end of the thigh-bone [femur] is made in the manner of a spout or gutter, & ...the head thereof is verie smooth and slipperie"3. He goes on to note that the joint is 'more lax' than the elbow and is therefore easier to dislocate. However, like Hippocrates, he says that it is easy to put back into place.
The signs of a dislocated knee are similar to those found in general dislocations: "Proturberance in the one part [where the dislocated head of the Fibula sticks out], and Cavity on the contrary."4 Sea surgeon James Handley adds that the "motion [of the leg] is weakened, and the figure is depraved."5 Paré includes a "disability of bending or lifting up the leg to the thigh, so that the patient cannot touch his buttock with his heel."6
Paré is the only surgeon to comment on causes for a dislocated knee. He mentions "Falls from high, leaping, and too violent running"7.
1 See John Woodall, the surgions mate, 1639, p. 155; 2 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 496; 3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 395 (mispaginated); 4 Wiseman, p. 496; 5 James Handley, Colloquia Chyrurgica, 1705, p. 161; 6,7 Paré, p. 395 (mispaginated)
Extending and Replacing a Dislocated Knee
Procedures for relocating the bones of the knee are fairly simple. Sea surgeon James Handley says "Let two Assistants make extension, one above, and the other below the Knee, near the Foot; and you must at the same time force the Bone into its place"1. Fellow sea surgeon John Atkins basically says to push the bones back in the way they came out.2 Both Richard Wiseman and Ambroise Paré note that dislocations to the side are easily restored "by a moderate Extension with your Hands."3
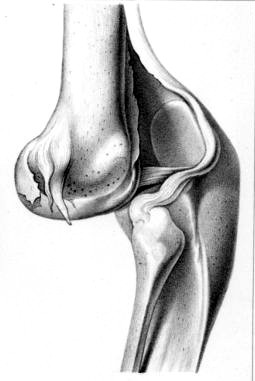
Knee Dislocated Backward, From Ouvrage:
Traite
des fractures et des luxations,
By Joseph
Francois Malgaigne (1855)
The backwards dislocation of a knee is a little more challenging. Atkins says "you are to have an Assistant for the Contra-Extension [pulling the part above the dislocation away from it] above the Knee, and yourself with one Hand on the Calf, and the other above the Ancle, are to extend forwards the Buttock, and it will knap in"4. Wiseman advises that the extension be made by bending the dislocated lower leg "suddenly backward, bringing his Heel to his Buttock"5, which is the same basic procedure as Atkins, albeit a bit more violent. Paré follows suit, although he says the patient should be seated on a bench first with the surgeon positioned behind him to bend the knee all the way back.
If that doesn't work, Paré offers another procedure, using a ligature, pole and ball:
make a clew [ball] of yarn, and fasten it upon the mid’st of a staff, let one put this into the cavitie of his ham [muscle at the back of the thigh], upon the place whereas the bone stand’s out, and so force it forwards; then let another cast a ligature of som three fingers bredth upon his knee, and draw it upwards with his hands, then presently & at once they all shal so bend and crook the lame leg that the heel thereof may touch his buttocks.6
Of course, with the exception of the three simple devices used to hold the leg steady and protect it, this is the same procedure as discussed by Atkins and Wiseman. No one shows an image of this form of relocation, although from the image of the backward dislocation, it is easy to see how pulling the lower leg suddenly back and up toward the buttock cause the bone to 'knap in'.
Wiseman offers a more intricate example of a cure for a perfect luxation (as opposed to a subluxation) in a case study. There, he had the patient lay on the side without a dislocation "then one of the company held him down, and kept that Thigh steady, whilst I took him by the foot and Calf of his Leg: and after I had a little drawn it to me, I forced it backward towards his Buttock, by which very motion it knapt into its place."7 However, this is again the same procedure, just performed with the patient in a different position.
1 James Handley, Colloquia Chyrurgica, 1705, p. 161; 2 John Atkins, The Navy Surgeon, 1742, p. 111; 3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 395 (mispaginated); 4 Atkins, p. 111; 5,6 Paré, p. 395 (mispaginated); 7 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 496
Securing the Knee and Post-Operative Care
Surgeon's Mate Spreading Plasters, From Hondert en
Dertien
Gebreken, By Jacques Guillemeau, Frontispiece (1678)
Once the dislocation had been corrected, medicines were applied to the site. For subluxated knees, Richard Wiseman advises astringent medicines. These cleanse and contract the body's tissues. However, in his case study of a perfect luxation of a knee, he becomes more expansive. "I embrocated the Leg cum albumine ov. [egg white] ol. ros. [oil of roses], myrtill [oil of myrtles], & aceto [vinegar], and applied empl. é bolo [a plaster containing oil, litharge or elemental lead, and bole or argillaceous earth] over all, with a Compress in his Ham"1. Of course, these are all just different types of astringents, so all he really did was spell them out. Sea surgeon John Atkins recommends his usual combination of oil of St. John's wort and oil of roses along with "a corroborative [strengthening] Emplaister on Kid Leather"2.
To bandage the repaired knee, Wiseman mentions in his case study that he "rowled it up, and laid his Leg upon a Pillow to the ease of the Patient."3 Atkins is more descriptive, advising the use of "a Compress in the Ham, a [piece of] Flannel over that, and then a double Rowler."4 He notes that the compress is used here both to keep the bone from prolapsing as well as to keep "the Tendons behind from Cold and Uneasiness, which too aptly contract them in these, as also in Fractures, that necessitate a long and inactive Confinement."5 This is clearly why he puts a piece of flannel over the compress.
Dressings for Luxated Knee, From A
Description of Bandages
and Dressings,
By Charles Gabriel Le Clerc, p. 80 (1701)
For the configuration of the bandage, we turn to Charles Gabriel Le Clerc. Like Atkins, he recommends a compress and roller bandage, although he doesn't mention the flannel. Since Atkins refers to Le Clerc's book several times when discussing the bandaging of dislocations, this should not be surprising. Le Clerc begins with a compress (1) "about an Inch thick, to lay under the Ham [back of the thigh], to hinder the Bandage from pressing on the Blood-Vessels, and Tendons; one end of this Compress must advance under the Thigh; and the other under the Leg, and be large enough to embrace the Ham"6. A surgeon's assistant was to hold the compress in place while the next piece, the roller bandage (2) was applied. This was an inch and half wide and about fifty-four inches long. The center of the bandage was set just above the luxated knee and rolled around to the front, just under the knee cap. There, the bandage was to "make an X above the Knee, approaching a little to it, so as to cover it by degrees; descend under the Ham, and make an X on the Leg, approaching thus gradually with X's over the Knee, till it be covered, then faften your Roller with several Rounds above the Knee."7 Le Clerc also mentions the use of junks - rolled up pieces of cloth with stiff, grass-like plants inside them so that they serve as splints.
Richard Wiseman has several ideas about long-term care of the healing knee in his case study, most involving resisting humors from getting to the relocated knee joint. He advises using "an Emulsion [mixture] of [oil of] the cold Seeds"8. There were four greater cold seeds - citrullus, gourd (cucubita), cucumber and muskmelon - and four lesser cold seeds - chicory, endive, lettuce and purslane. These were believed to have cooling abilities, so were appropriate for application to 'hot' health problems. (This draws upon the humoral property of medicines and illnesses, which is explained in detail here.) Cooling seeds were also thought to have opening and cleansing properties, which helped to purge bad humors from the system.
Wiseman goes on to recommend other medicines in his case study. On the third day, he repeated the application of cold seed oil, adding vinegar "and thereby repelled the Humour so, that there only remained some remarques [indications] of the extravasated [leaking] blood."9 After this, he "embrocated those Parts cum ol. cham.

Artist: Jan Luyken - Working the Leg, From Het Menselyk (1694)
[oil of chamomile] lumbric. [oil of earthworms] spir. vini [spirit of wine], and applied empl. stict. Paracels. [Paracelsus plaster] & diapalmæ [diapalma plaster] on the weak Joint."10 Several other humor-purging procedures were recommended by Wiseman including letting blood, administering clysters or enemas and a 'slender' Diet, which was felt to decrease the production of unwanted humors in the body.
Due to the ease with which it dislocates, Atkins discusses the possibility of the joint prolapsing when the muscles and tendons contract. If this occurred, the surgeon was to use "warm and emollient Embrocations and Fomenting, [and] a Working of the Limb backwards and forwards on the Joint"11. He explains that the muscles and tendons "soften, and unbend with Warmth, Moisture and Motion... I knew such a Contraction of the Flexors, and a long Confinement for a Fracture of the Leg, that when Ointments and Fomentations had been used to no Purpose, unbended and straitened after about a quarter of an Hour’s such Exercise with the Limb."12 Once again, we have an example of physical therapy being used on dislocated joints during the golden age of piracy.
1 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 496; 2 John Atkins, The Navy Surgeon, 1742, p. 111; 3 Wiseman, p. 496; 11 Atkins, p. 112; 5 Atkins, p. 112; 6 Charles Gabriel Le Clerc, A Description of Bandages and Dressings, p. 80-1; 7 Le Clerc, p. 81; 8,9,10 Wiseman, p. 497; 11,12 Atkins, p. 112
Specific Dislocation/Luxation Cure: Ankle
The ankle is one of the two dislocations mentioned by all the authors under study, the other being the shoulder. As he did with several other luxations, sea surgeon John Woodall only mentions it as something that can easily be repaired with his device the commander.1 All the other authors have more to say on repairing an ankle dislocation. Sea surgeon John Atkins advises that because the ankle joint is so "fast bound with Membranes, Ligaments, and Tendons, makes it very difficult of Luxation."2 While English surgeon Richard Wiseman agrees with his assessment in theory, he explains that the ankle "would not easily be dislocated, did not so great a weight lie thereupon."3

Image: James Hielman - Forward Dislocation of the Ankle
The ankle can be dislocated inward, outward, forward and backward. Everyone attempts to explain the symptoms of each type of ankle dislocation by its appearance, but most of them are more confusing than helpful. Sea surgeon James Handley gives the most cogent explanation:
If it be Dislocated inward, the sole of the Foot turns outward, and if dislocated outward, it turns the contrary Way: if forward, the broad Tendon of the Heel... is, torte [taut] and hard, and the Foot is less [shorter than normal]: if the Dislocation be backwards, the Heel is almost hid, the sole of the Foot seems bigger, and the Foot longer.4
Atkins adds that the more perfect or complete the luxation is the more likely it will suffer "insupportable Pain, a long and tedious Weakness, and sometimes irrecoverable Lameness."5 However, he also warns that such symptoms are present in ankle sprains, but since "it is not easy to perceive any small Distortion of the Bone through a large Tumor, or a peculiar Conformity; I say, in regard to this, it is not implolitick to recommend Extension at all times"6.
French surgeon Ambroise Paré says that ankle dislocations do not "happen without much violence"7. Atkins, on the other hand, notes that partial ankle dislocations can be caused by 'slight accidents' "such as slipping on an uneven Surface, sudden Stumbles and Falls"8. Although he doesn't say so, it is likely that Paré is talking about complete dislocations while Atkins specifically says he is talking about partial dislocations.
1 John Woodall, the surgions mate, 1639, p. 155; 2 John Atkins, The Navy Surgeon, 1742, p. 114; 3 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 497; 4 James Handley, Colloquia Chyrurgica, 1705, p. 161; 5,6 Atkins, p. 115; 7 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 395 (mispaginated); 8 Atkins, p. 115
Reducing and Caring For a Dislocated Ankle

Artist: after Adriaen van Ostade - surgeon Working With a Man's Foot (17th c.)
Although everyone talks about ankle dislocations, their comments on restoring them are quite brief. Sea surgeon James Handley simply says ankle reduction is performed "[b]y good Extension and Reposition, and cured as other Luxations"1. English military surgeon Richard Wiseman expands on this a bit, noting that restoration of a dislocated ankle "may be [made] by Extension with your hands the one taking hold of the Leg, the other of the Foot. During which Extension, The Chirurgeon must press the Bone the contrary way to which it was fallen."2
Sea surgeon John Moyle combines the method for extending a dislocated wrist with that of the ankle. He recommends having three people, with the two assistants making extension and counter-extension of the joint while the surgeon replaces the bone.3 Even the normally expansive French surgeon Ambroise Paré only says "It is restored by extending it with the hands, and forcing it into the contrary part to that from whence it fell."4
Sea surgeon John Atkins provides the most extensive explanation of reducing a dislocated ankle.
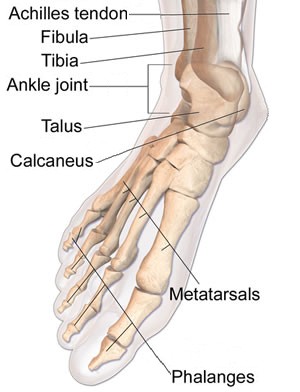
Image: James Hielman - Forward Dislocation of the Ankle
Extension should be made with one Hand on the Metacarpus [probably meaning the metatarsels], the other on the Heel, while an Assistant holds the Leg the same Time: Having collected from the aforegoing Signs, how the Head of the Astragalus [Talus] lies distorted, wring the Foot the contrary Way; or when the Recession is small, or but suspected, press gently with your Fingers about the Joint, (when at its Extension,) to restore the Deformity.5
Wiseman adds a last thought on reducing a dislocated ankle. "In case the Extension by your Hands suffice not, you may make use of Pulleys or other Engines."6 He doesn't give any further details, although Woodall's beloved commander comes to mind.
Once restored, "it is kept so by application of medicines and fit ligation."7 (That is all that Paré has to say about medicating and bandaging the ankle.) Wiseman again suggests restrictive medicines for this dislocation8 as he did for elbow and hip dislocations. These were probably recommended to prevent humors from gathering at the site. Moyle recommends the same thing he did for dislocations of the hip: "embrocate with Ol. Rosarum [oil of roses], and apply the defensive Plaster [most likely referring to his defensivum minor]"9 As with the other areas of healing an ankle dislocation, Atkins has the most to say on the subject of medicines. "The Cure consists in the present, and continued Use of the Cold Bath, an Embrocation of Ol. Rosar. [Oil of Roses] Hiper. [oil of St. John's wort] p. ae. [in equal quantities] a Corroborative [strengthening] Empl. Ex Minio [red lead plaster] & Diapalm. [Emplastrum Diapalma]"10.
Very little is said about the way to bandaging a dislocated ankle. Atkins notes that a roller bandage should be used, but he gives no details. This may be because his go to source for bandaging, Charles Gabriel Le Clerc's book, has nothing to say on the topic.

A Metal Leg Brace from Lorenz Heister's
Book A General System of Surgery,
Plate 36 (1750)
However, the dressing of a dislocated ankle is the one place where sea surgeon Hugh Ryder provides some truly interesting comments. He had a patient with a dislocated ankle that he explained couldn't be remedied. To help the patient, he made "an
Instrument of Steel riveted to the Shoe below, and coming up to the outside of the Leg, with a Leather Brace at the gartering place [mid-calf], and another below, to Lace on the out-side of the outer Ancle by which means the head of the Bone was firmly kept in his place and he went indifferently [moderately] well."11 Writing in 1957 about the history naval medicine, historian John Keevil points out that Ryder's "improvisation supplies the origin of an orthopaedic treatment still in use today."12 Atkins suggested a similar solution: "a sort of half Boot, coming up as a Part of the Shoe to lace on, and steady the Joint."13
For long-term care, everyone recommends bed rest. Sea surgeon Moyle advised that the patient should "not stir that part too much; and ...not endeavour to go or stand upon it until ‘tis well."14 Fellow sea surgeon Handley suggested he 'keep his Bed' at least thirty or forty days to prevent it from become dislocated again.15 Sea surgeon Atkins recommended "the properest Ingredient towards Amendment, resting on a soft Pillow."16 Paré closes out the chorus of votes for bed rest by explaining "that bone which sustain’s and bear’s up the whole body, may again sink under the burden, and break out, the sinews beeing not well knit and strengthened."17
1 James Handley, Colloquia Chyrurgica, 1705, p. 161; 2 Richard Wiseman, Severall Chirurgicall Treatises, 2nd ed., 1686, p. 497; 3 John Moyle, Chirugius Marinus: Or, The Sea Chirurgeon, 1693, p. 125; 4 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, 1649, p. 397 (mispaginated); 5 John Atkins, The Navy Surgeon, 1742, p. 115-6; 6 Wiseman, p. 498; 7 Paré, p. 397 (mispaginated); 8 Wiseman, p. 498; 9 Moyle, p. 125; 10 Atkins, p. 116; 11 Hugh Ryder, New Practical Observations in Surgery Containing Divers Remarkable Cases and Cures, 1685, p. 72-3; 12 John J. Keevil, Medicine and the Navy 1200-1900: Volume II – 1640-1714, 1958, p. 169; 13 Atkins, p. 116; 14 Moyle, p. 125; 15 Handley, p. 161; 16 Atkins, p. 116; 17 Paré, p. 397 (mispaginated);
Treating Sprains and luxations Page Menu: 1 2 3 4 5 6 7 8 9 10 11 12 13 Next>>
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-