

Needle and Suture Pages: 1 2 3 4 5 <<First
Needles and Suturing in the Golden Age of Piracy, Page 5
Suturing Procedures: When Not Sutured
Pierre Dionis was a proponent of suturing in many cases, explaining that "Sutures are infallible Means of the closure of the Wounds, and procuring their Re-union", yet he also identified seven situations where stitching was specifically not to be used. These included:

Photo: Wes Washington
Contused Wound, Unsuitable for Suturing
- Wounds suspected to be invenom’d, because ‘tis proper to provide an Issue [intentionally made abcess] for the Poison, and to conduct the Remedies [medicines] to the Interior of these Parts, to which the Venom has insinuated it self
- [I]n Wounds of the Breast, by reason of its continual Motion [Referring to the motion of the lungs inflating and deflating cause the breast to move.]
- In those accompanied with violent Inflammations, because the point of the Needle would yet increase them
- [I]n Contusions [bruised skin], the Flesh not being firm enough to bear the Thread
- [I]n these Wounds attended with the Aperture of the great Vessels [veins and arteries which bring blood to and from the heart], which are to be closed by Ligature [tying off] or Astringents [medicines to stop bleeding]
- [I]n those [wounds] which discover [uncover] the Bones, by reason of the exfoliation [casting off of necrotic bone matter] which is to be expected [The exfoliated bone matter must have a way out of the body]
- [I]n Wounds accompanied with a signal [notable] loss of Substance, because ‘tis necessity to draw out the Pus or Matter, in order to the Regeneration of the Flesh.1
Sixteenth century military surgeon William Clowes, also a proponent of suturing, warned of several similar situations where sutures were problematic. He advised they not be used for "small wounds in the face, or bruised wounds, where the stitches will rot out, or in venomous bitings, or where the wound that is stitched tends to imposthumation [formation of pus], there to cut open the stitches I hold it profitable"2.
Closing a deep wound with the potential for ejecting matter (Dionis' 7th point and the last one mentioned by Clowes) was agreed to be a bad idea by several period surgeons. Ambroise Paré explains that when you suture such a deep wound "you only take hold of the upper part, the Wound is superficially healed: but the matter [is] shut up, and gathered together in the bottome of the Wound, [which] will cause abscesses and hollow Ulcers"3.
Of course, leaving an opening in a suture could be done with adroit stitching. In at least one instance, Clowes sutured a wound while still "leaving a decent place for the wound to purge at"4. Richard Wiseman similarly said that "if the Wound be so deep as you suspect its incarning [formation of new flesh] in the bottom, you must leave a declining Orifice [opening into the wound] for the discharge of Matter."5
1 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 40; 2 William Clowes, Selected Writings of William Clowes, p. 111; 3 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, p. 255; 4 Clowes, p. 108; 5 Richard Wiseman, Of Wounds, Severall Chirurgicall Treatises, p. 349Suturing Procedures: Post-Suture Medicines
Two different medicines were recommended for topical application by period surgeons after a wound was sutured. The first were agglutinative medicines and and the second were medicines designed to nourish the wound.
Agglutinative medicines were applied after stitching was completed; they contained elements that caused the lips of the wound to adhere to each other. After stitching a wound, English military surgeon William Clowes said he used "Oleum hyperici cum gummo [St. John's wort mixed with gum - possibly gum arabic], and I stayed the bleeding with Galen his powder." French surgeon Ambroise Paré explained that agglutinative medicines "ought to be indued with a drying and astrictive [astringent] quality, whereby they may hold together the lips of the wound, and drive away defluxion [flows of humors into the wound], 
Vial G, From
Pierre Dionis, Fig
VIII,
p. 59 (1740)
having alwayes regard to the nature of the part and the greatnesse of the disease."2

Photo: Petr Filippov
Rough and Branched Horsetail (Equisetum)
French surgical instructor Pierre Dionis recommended a agglutinative powder called 'the Conservatrix of Sutures' which was "composed of glutinous [glue-like] and viscous Ingredients, such as Mastick [mastic - mastic tree resin], Myrrh, Bolus [an aggregate of herbs, probably clays or gums], and Aloes; of this Powder there is some in the Vial G."3
Paré detailed a number of agglutinating 'simples' - medicines not combined with other ingredients. These included "Olibanum [aromatic gum resin obtained from various Arabian or East African trees], Aloes, Sarcocolla [a gum resin from plants discussed in the section on wound glues], Bole-Armenick [a red astringent clay], Terra sigillata [reddish-brown clay used as a general cure for any bodily impurities], Sanguis Draconis [Dragon’s Blood, a red vegetable gum, promotes tissue growth, reduces ulcers], Common and Venice Turpentine, Gumme Elemnii [gum resin, used for stimulating ulcers], Plantane, Horse-tayle [Equisetum], the greater Comfery, Farina Volatilis [flour of wheat, used for making cataplasms], and many other things of this kind"4.
Military surgeon Richard Wiseman suggests an emplastic, another name for an agglutinative medicine which contains a variety of substances similar to those already mentioned. His prescription is "Rx bol. Armen. {3 ounces} sang. dracon. [Dragon’s Blood] thuris [frankincense], aloes, glutin. sicc. [dried gluten] an. [ana - of each] {1 ounce} 
Pierre Dionis, Fig
VIII,
p. 59 (1740)
gypsi [gypsum or Plaster of Paris], farin. volatilis [finely ground wheat flour], an. {half dram} hypocistid [the juice of Cytinus hypocistis]. acatiæ [juice of sloes], sumach. [poison oak leaves] an. {3 ounces} Misc. cum album. ov. [mix with egg white] to the consistence of Honey, and apply over it a Compress squeezed out of Oxycrate [water and vinegar] or Red wine"5.
Dionis notes that some authors advise the use of a "nutritive Juice, which is repairing to the Part, procures the Reunion."6 He specifically suggests that "Arcæus’s Balsam, which is in the little Pot H, is commonly used"7. Franciscus Arcæus was a Spanish surgeon of great renown practicing in the 16th century. His balsam contained a mixture of turpentine, gum-elemi, suet and lard.8
1 William Clowes, Selected Writings of William Clowes, p. 108; 2 Ambroise Paré, The Apologie and Treatise of Ambroise Paré, p.126; 3 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 42; 4 Paré, ibid.; 5 Richard Wiseman, Eight Chirurgicall Treatises, 3rd Edition, p. 353; 6,7 Dionis, ibid.; 8 Society for the Diffusion of Useful Knowledge (Great Britain), The Biographical Dictionary of the Society for the Diffusion of Useful Knowledge, Vol. 3, Issue 1, 1843, p. 263
Suturing Procedures: Post-Suture Bandaging
Dionis provides a detailed explanation of how a sutured wound was treated after being medicated. Once the medicine is applied,
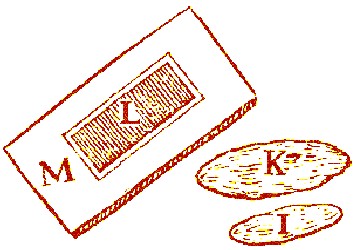
Suture Dressings, From Pierre Dionis' Cours d'Operations,
Fig VII, "Of Sutures", p. 59 (1740)
the small Pledget I is charged [medicated] and clap’d on the Suture, and afterwards covered with the great Pledget K, which is large enough to extend over the Knots [of the suture], to the end that the Plaster not sticking to them, the Dressing may be taken off without pain. Next is laid on the Plaister L, which ought to be composed of viscous and astringent Ingredients, such as that for Ruptures; then the Bolster M, moisten’d in some Liquor which fortifies and resists Putrefaction.
As for the Bandage, it ought to be conform’d to the Figure of the wounded Part, for which reason it cannot be particularly specified, but it must be so perform’d as to retain the Lips of the Wound closely join’d together.1
English military surgeon Richard Wiseman recommends a much simpler dressing once the stitching is complete and agglutinative medicines have been applied. He advised the surgeon to "rowl up the Member with the agglutinative Rowler, beginning on the opposite part, bringing both the heads over the Wound: and having taken a turn or two there, rowl upwards and downwards, so as to press the bloud upward, and restrain the Influx from above. Your Bandage must be so made, that it be to the ease of the Patient: the Position ought also to be such as may prevent Pain."2
1 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 42; 2 Richard Wiseman, Eight Chirurgicall Treatises, 3rd Edition, p. 353
Suturing Procedures: Suture Removal
"When a Wound is Re-united, the next Task is to take off the Suture; in order to the performance of which with Prudence and Address". (Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 44)
Two surgeons from the period discuss the removal of sutures. The ever detail-oriented French instructor Dionis explains that the surgeon knows it's time to remove the stitches "when he finds the Wound perfectly well cur’d;
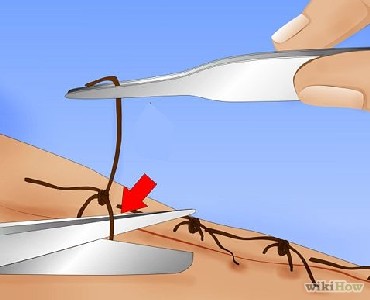
Removing Incarnative Sutures with Scissors and Forceps (instead of
a probe), From the
Wiki How article "How to
Remove Stitches"
when there is nothing left to cicatrize [heal] but the small Stitches made by the Needle, which always keeping those Holes open prevents their closing [and properly healing]"1.
Richard Wiseman advises his readers that "you must use your judgment: for sometimes the Wound may seem to be agglutinated [glued together], while the Lips are held together by Suture, which, after the Stitches are cut out, is not so exactly cicatrized [healed], but that you might have done better to have left the Stitches a day longer."2
Dionis explains the method for removing through-skin stitches depends on the type of stitch that is being removed. For Incarnative sutures, "a small Probe ought to be run under the Thread, after which is must be cut near the Knot on the Probe, and afterwards in drawing it out by the Knot the Finger must be kept on the Wound in such a manner as to prevent its opening again"3.
For Threaded sutures, "the Thread around the Needles is unwound, and the Needles dexterously drawn out; taking care that it is done without Violence, for fear of renewing the Wound"4.
When the glover's stitch is removed, Dionis simply says that it must be "pulled or unspun, that it may not hurt [the wounded part - in this case the intestines or Epiploon - membrane lining the abdominal cavity] when they happen to rase [rub] against it."5
1 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 44; 2 Richard Wiseman, Eight Chirurgicall Treatises, 3rd Edition, p. 345; 3,4 Dionis, p. 44; 5 Dionis, p. 57
Suturing Procedures: Specific Uses
Although this article has noted that stitches were not as widely used during the golden age of the pirates as they are today, they still enjoyed a fair amount of popularity. Several period surgeons talk using stitches as an important part of various specific cures they performed. Let's look at some of these.
Wound closure was obviously an important use of suturing. Ambroise Paré advised,
Artist: Eduoad Jean Conrad Hamman
Paré Treating Wounded Soldiers (19th century print)
When Wounds are made alongst the thighs, legs, and arms, they may easily want Sutures, because the solution of continuity [the tear in the flesh] is easily restored by Ligatures [material used to bind the wound tightly], usually to stop bleeding], but when they are made overthwart [across], they require a Suture ...that they may be joyned and so kept, they must be sowed, and if the Wound be deep, you must take up much flesh with your needle1.
Richard Wiseman gives some specific insight into how to prepare wounds that weren't dressed quickly enough to keep the wound edges from hardening. "If the Wound hath lain long undressed, or were not stitched at the first dressing, and be now so contracted and stubborn that the Lips of it will not be brought near one another; you must then foment them warm with some lenient Decoction ex fol. & rad. Althææ [root of marshmallow], malvæ [malva plant], viol. [violet] sem. lini [crushed linseed], &c. or with new Milk; then joyn them together, as hath been said, and dress them as Wounds so stitcht."2
Open gunshot wounds were also sutured when they were large enough to require it. When discussing gunshot wound treatment, sea surgeon John Woodall tells the surgeon's assistants to have "good Ligature [thread] of all sorts, stitching needles ready, with all other fit instruments not farre off"3.

Nose Surgery, From Cheirurgia nova, By Gasparo
Tagliacozzi, Fig. 11, p 582 (1598)
Another specific case for stitching was for reattaching partially severed body parts. Ambroise Paré gives quite a bit of detail on the suturing required in such cases. He advises that when "a fleshy substance by reason of some great cut shall hang downe, it must necessarily be adjoyned and kept in the place by suture." He said that such wounds occurred to body parts such as "the Eares, Nose, Hairy-scalpe, Eie-liddes, Lippes, Belly and Throat."4
Paré provides some detail on suturing a partially severed ear. He explains that in such a case "it is fit to use a suture; but yet so that you touch not the gristle [cartilage] with your needle; for thence there would be in danger of a gangræne which happens by foolish curing; therefore you shall take up and comprehend with your needle only the skin, and that little flesh which encompasses the gristle. You shall perform the rest of the cure with pledgets and ligatures artificially fitted, and shall resist inflammation and other symptoms with fit medicins."5

Suturing the Stump, From The French Chirurgerie. By Jacques
Guillemeau, p.29
A third specific case involving suturing was during amputation. While it may not not surprising that the end of the amputated stump was sutured, the way in which it was done is curious by today's standards. Rather than suture the remaining skin over the end of the stump finely, John Woodall explains that some period surgeons used "two great square stitching needles armed with very strong thred waxed"6.
The skin of the amputated limb was usually cut so that it was longer than end of the stump. Woodall advised the surgeon to "stitch the skin through on the outside and just over the other side, and with the other needle doe likewise as it were crosse over the member the other way, and draw the said threds so close as you thinke convenient, the better to stop and choake the great Veynes and Arteries, then tye them fast"7. This is not the fine suturing of skin we think of with wounds; it is only two thick threads used to pull the skin over the amputated stump in the pattern of an 'X'. Its primary purpose wasn't really to bring the wound edges together so much as it was to stop bleeding.
A final specific case discussed by period surgeons in great detail was the repair of intestines exposed by stomach wounds. John Woodall noted that stomach wounds were pretty much treated like other wounds for the most part. It was "onely in stitching they differ much,

Artist: Gaspare Traversi
Intestinal Wound Treatment, The Operation (1753-4)
but the inward differ, as the parts offended may be divers [many]". Here he lists a variety of abdominal complications that can occur in such wounds, most of which have little to do with suturing. However, Woodall does advise that "if the substance of a gut [referring to the intestines] be wounded, sow it together and consolidate it"8.
Ambroise Paré prescribes gold or other metal sutures for the intestines, as was discussed previously in the section on needles and Punctus Aureus. However most surgeons used cloth or silk sutures.
Richard Wiseman says that if "the Omentum [peritoneum or lining the abdominal cavity] be slipt out and tainted by the Air, make a Ligature above the solid part [which is hanging out of the wound], and cut it off; then stitch up the Wound, leaving then ends of the Ligature hanging out of it to cast off. But it if be fresh and warm, reduce it [put it back inside] with your fingers."9
The ever-thorough French surgical instructor Pierre Dionis gives detailed instructions on how to heal wounds of the intestines. He first advises the surgeon to locate any tears in the intestines by carefully pulling them out enough to examine them. "When [the wound] 'tis very little, or not larger than a Wound with a Bodkin or Penknife, 'tis needless to sew It; Nature, seconded [supported] by a very exact Diet, is able to cure it; But if it be large, as those made by the thrust of a Knife or Sword, or there be two or three, as sometimes happens, the Furriers Suture [Glover's stitch] is to be apply'd."10
Wiseman concurs, ordering his readers to "stitch the Gut with the Glovers Stitch, sprinkling it with some of the aforementioned Agglutinates [mastic & lumbric]; and reducing it back [putting it back in place], stitch up the external Wound of the Belly, as hath been said."11
Dionis gives a more detailed procedure for repairing the wounded intestine:
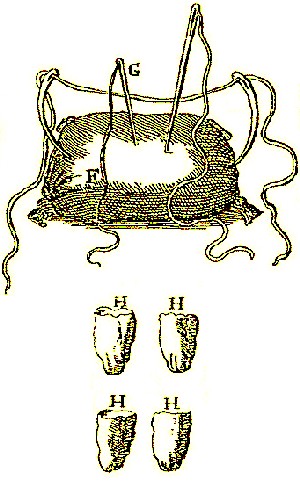
Tools For Suturing Intestines, From Pierre Dionis' Cours
d'Operations, Fig IX, p. 49 (1733)
The Chirurgeon commonly takes raw flat Silk, F; it must be flat, such as Women use in their working Tapistry, that each Stitch being the broader, may the better stop the Aperture of the Wound; it must be raw, that is, not dyed, because several Drugs enter into the Dyes, which might envenom the Wound by moistning it with them: He makes use of the Needle, G, which is straight and round, for the Reasons I have already hinted.
There are prepar'd four Thimbles, or Finger-stalls made of Linen, H H H H; two of which serve to put on the Thumb and Fore-finger of one of the Servant's Hands, and the other two for the Thumb and Fore-finger of the Chirurgeon's left Hand: These thimbles are used to prevent the Intestines slipping through the Thumb and Fingers with which 'tis held, which 'twould certainly do without them.
The Operator takes in his right Hand the Needle threaded with the Silk, and runs it across the two Lips of the Wound at a higher place, and a little below makes a second Stitch in the same manner, not forgetting to twist the end of the Silk under the second Stitch, rather than knot it: he continues on as many Stitches as the length of the Wound requires, and leaves betwixt each the distance of about the thickness of a Crown Piece, ending by a Stitch beyond the end of the wound, as he began a Stitch beyond its Circumference, that it may be sewed up so exactly close, that there remain no small Orifice through which any thing may escape; and at last he fastens or twists the Silk at the last Stitch, that he may not be oblig'd to tie any Knot.
'Tis, by way of Caution, recommended to the Operator, to leave out, at the Wound of the Belly, an end of the Silk about a Foot long, after the Intestine is put in again, that he may have it in his Power to draw it [the silk thread] out, when the Wound of the Intestine being cicatriz'd [healed], it becomes intirely separated from it; this is a part of the Practice which must not be omitted; it is customary, at the finishing of the Suture, to cut the Silk close to the Needle, and leave the end of it at the end of the Suture.12

Mastic Tears Arabic Gum
Dionis explains that "Some Authors order a little pulveriz'd Mastic [plant resin] to be laid on the Suture, in order to conglutinate [join] it the sooner; but... I advise the returning in the Intestines the first Moment possible, because the natural Heat of the Belly will do them more good than all the Remedies which can be apply'd."13
This is only the first part of the operation in Dionis' explanation. The second part involves sewing the wounds in the periosteum and skin which allowed the intestines to come out. First the surgeon is to check to make sure the membrane of the epiploon (or the periosteum membrane which covers the intestines) has not decayed while outside the body. If it has, it must be tied off so that the putrefied parts can be removed. The surgeon
takes a coarse waxed Thread, or small String I, at the end of which he has a straight Needle, K, threaded. He draws the Epiploon a little farther of the Body than it is already, that he may not make his Ligature upon that which is corrupted; he then binds this Membrane twice or thrice round the sound part with the String, drawing the Ligature moderately tight, for fear, lest if too hard, it should cut in the performance, or in leaving it too slack, the Vessels which are very numerous should pour out their Blood in the Cavity of the Belly.
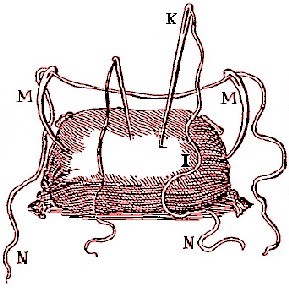
Tools For Suturing Omentum & Abdominal Skin,
From Pierre Dionis' Cours d'Operations, Fig IX,
p. 49 (1733)
He runs the Needle through across the proper Substance of this Organ [the epiploon], that the Ligature may not slip; then he cuts it off within half a Finger's breadth of the Ligature, leaving out of the Body an end of the String as long as that of the Silk, to draw it out when the Scar is fallen off. Next he puts the Epiploon into the Belly; and, in order to enable him to extend it over the Intestines, which is its natural Place, he a little moves and shakes the Patient...
After having put into order the Intestine and Epiploon, a Servant should with both Hands hold the two Lips of the Wound in the Abdomen close to each other, that the Organs may not fly out, whilst the Chirurgeon disposes himself to perform the Suture of the Belly.... The Chirurgeon must have two large Curve Needles, M, M, threaded with the String N, which is better than Thread, because being coarser it will not cut the Lips of the Wound. He puts his Fore-finger into the Wound, in order to hold the Peritoneum, the Muscles and Skin together; then with the other Hand he thrusts one of the Needles thro' into the Belly, guiding the Point on his Fore-finger, to avoid pricking the Epiploon or Intestines: he pierces from the inside outwards one of the edges of the Wound far enough forwards, that the Suture may hold the better, and resist the continual Motion of the inferior Venter [underside of the abdomen]; and having drawn out his Needle on the outside, he takes the other Needle, with which he pierces the other side of the Wound in the same manner, and with the same Precaution as at the first Stitch, observing, that if he held the first Needle in the right Hand to run the Thread from the Right to the Left, he ought to draw the second thro' from the Left to the Right with his Left Hand.14
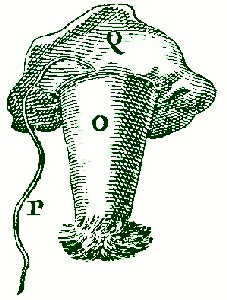
Abdominal Tent,
From Pierre Dionis' Cours
d'Operations,
Fig IX, p. 49 (1733)
Dionis is using the Incarnative suture as he does on skin of other parts of the body, only he is doing it with two needles at once. He notes that stitches "ought to be [placed] closer to each other in Sutures of the Belly, than in those of any other part, by reason of its motion"15.
Dionis inserts an interesting step before closing this wound. He says that "before knotting of the [suture] Strings, a large Linen Tent O, ought to be applied to the lowest part of the Wound, and to the head of this Tent must be fastnen'd a Thread P, tho' it has a Head Q, made of the same Linen, for fear lest it should sink into the Abdomen. 'Tis very necessary there, as well because it secures a Passage outwards for the extravasated [forced out] Blood, Pus, and other exotic Bodies, as by reason that it keeps the Wound open 'till the Intestine and Epiploon are healed, when the Thread may be drawn out"16.
After the abdominal tent is in place, each stitch is tied off "by passing in the first Stitch the String twice thro' the same loop, which is called the Chirurgeon's knot, because it holds better than any other."17
1 Ambroise Paré, The Workes of that Famous Chirurgion Ambrose Parey, p. 255; 2 Richard Wiseman, Of Wounds, Severall Chirurgicall Treatises, p. 349; 3 John Woodall, the surgions mate, p. 142; 4 Ambroise Paré, The Apologie and Treatise of Ambroise Paré, p.126; 5 Paré, Workes, p. 295; 6 Woodall, p. 173; 7 Woodall, p. 173; 8 John Woodall, the surgions mate, 1655 edition, p. 94; 9 Wiseman, p. 363; 10 Pierre Dionis, A course of chirurgical operations: demonstrated in the royal garden at Paris. 2nd ed., p. 53-4; 11 Wiseman, p. 364; 12 Dionis, p. 54; 13 Dionis, p. 55; 14 Dionis, p. 55-6; 15 Dionis, p. 56; 16 Dionis, p. 56-7; 17 Dionis, p. 56
Needle and Suture Pages: 1 2 3 4 5 <<First
Main Page • Tools & Procedures • Miscellanea • About the Author • Facebook Page
All original content copyright M. Kehoe • 2003-